PRINCIPLES OF VETERINARY COMMUNITY ENGAGEMENT
Brittany Watson, MS, VMD, PhD, DACVPM
Director of Shelter Medicine and Community Engagement
Associate Professor in Shelter Medicine and Community Engagement, Clinician Educator (CE)
Department of Clinical Sciences & Advanced Medicine
University of Pennsylvania School of Veterinary Medicine, Philadelphia, PA
Elizabeth Berliner, DVM, MA, DABVP
(Shelter Medicine Practice, Canine & Feline Practice)
Senior Director, Shelter Medicine Services, ASPCA
Courtesy Associate Clinical Professor
Cornell University College of Veterinary Medicine Ithaca, NY
Lena DeTar, DVM, MS, DACVPM, DABVP
(Shelter Medicine Practice)
Maddie’s® Shelter Medicine Program
Associate Clinical Professor
Cornell University College of Veterinary Medicine Ithaca, NY
Emily McCobb, DVM, MS, DACVAA
Associate Clinical Professor of Anesthesiology and Community Medicine
Center for Animals and Public Policy and Department of Clinical Sciences
Cummings School of Veterinary Medicine
Tufts University
North Grafton, MA
William Frahm-Gilles, DVM
Access Veterinary Care
Minneapolis, MN
Erin Henry, VMD, DACVPM
Assistant Clinical Professor
Maddie’s® Shelter Medicine Program
Cornell University College of Veterinary Medicine Ithaca, NY
Erin King, MS
Civic Life Coordinator
Jonathan M. Tisch College of Civic Life PhD Candidate
Cummings School of Veterinary Medicine
Tufts University
North Grafton, MA
Lauren Powell, PhD
Lecturer in Animal Welfare and Behavior
Department of Clinical Sciences & Advanced Medicine, University of Pennsylvania School of Veterinary Medicine
Philadelphia, PA
Chelsea Reinhard, DVM, MPH, DACVPM, DABVP
(Shelter Medicine Practice)
Bernice Barbour Assistant Professor of Clinical Shelter Medicine
Department of Clinical Sciences & Advanced Medicine
University of Pennsylvania School of Veterinary Medicine, Philadelphia, PA
Jenny Stavisky, MRCVS, BVMS, PhD, PGCHE FHEA
Clinical Research Manager
Vetpartners, UK
Citation: Journal of Shelter Medicine and Community Animal Health 2024 - http://dx.doi.org/10.56771/VCEprinciples.2024
Copyright: © 2024 Author(s). This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Published: 12 September 2024
Acknowledgements
The authors thank Peter Javian for assistance with the logistics and compilation of this document. We would also like to thank Kirsten White, who helped compile the glossary, and Karen Verderame for assistance with distribution. Both of these individuals contributed greatly to conversations regarding the formal feedback process and were key members of the development team. Padraig McCobb designed our graphical abstract.
The authors acknowledge the following individuals who provided edits and suggestions to the document. This document was significantly enhanced by their insights and assistance, and they were a critical part of the development process. This list only includes those individuals who elected to be recognized. There were many other individuals who are not identified here also contributed meaningful and helpful feedback to the authorship team.
Companions and Animals for Reform and Equity (also known as CARE)
National BIPOC Led Human and Animal Well-being Organization
https://careawo.org
Chumkee Aziz, DVM, DABVP (Shelter Medicine Practice)
University of California- Davis, Koret Shelter Medicine Program
Maya Gupta, PhD
Senior Director, Research
ASPCA
Lynn Henderson, DVM, MEd, CHPV
Veterinary Director, Kim & Stu Lang Community Healthcare Partnership Program
Ontario Veterinary College
Kristin Jankowski, VMD
Access to Care Veterinarian, UC Davis One Health Institute
Advisor, Knights Landing One Health Clinic, UC Davis School of Veterinary Medicine, Director of Veterinary Services, Open Door Veterinary Collective
Ronald J. Orchard, DVM, MPH, CAWA
Clinical Instructor of Community Outreach
College of Veterinary Medicine
Kansas State University
Karen Ward, DVM
Chief Veterinary Officer
Toronto Humane Society
Jennifer Weisent, DVM, PhD
Associate Clinical Professor, Shelter Medicine
University of Tennessee College of Veterinary Medicine
Windi Wojdak, RVT and Aleisha Swartz, DVM
Rural Area Veterinary Services
Humane Society of the United States
Executive summary
The concepts of One Health and One Welfare recognize the integral and complex relationship between animals, the environment, and human health. Pivotal events such as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) global pandemic and Hurricane Katrina have highlighted how integral animals are to families and communities; even in times of crisis, people rally to protect and care for their animals despite risks to their own well-being. Health inequities and social determinants of health are increasingly being recognized in the veterinary landscape, which has inspired many groups to initiate projects that support community members and their pets.
When engaging with the animals of marginalized, underserved, or underrepresented communities, the veterinary medical field has opportunities and responsibilities. Project volunteers are often excited and passionate, and if guided well, their efforts can have significant impacts on people and their animals. Unfortunately, good intentions do not guarantee positive outcomes. Our field has an obligation to identify and follow evidence-based ethical engagement practices refined through decades of research from human health engagement programs. As veterinary community engagement continues to gain momentum in academic and research settings, the public sector, philanthropic organizations, and veterinary student training programs, formal guidelines for such engagement have become necessary.
These Principles of Veterinary Community Engagement are closely adapted from the second edition of the Principles of Community Engagement, published in 2011 by a coalition of human health agencies to guide human healthcare programs. Our publication echoes their original principles and reflects their chapter titles and concepts but has been reorganized and refined to focus on programs providing healthcare services to animals.
Many types of animal-related engagement occur in communities. The scope of this resource is focused on programs providing animal health services in a community partnership, especially those involving veterinary care. The concepts described here may widely apply to other animal areas such as educational public and classroom outreach, animal-assisted healthcare, and human-animal interactions with service and therapy animals; however, these programs are not the primary focus of this document.
The intended audience for this document includes individuals designing, leading, and participating in veterinary community engagement programs. Interested parties include instructors, veterinary practitioners, academic institutions, governmental agencies, non-governmental organizations, community members, students, and field leaders who collaboratively help to ensure organizers are following best practices in public health and community engagement and minimizing harm to animal and human populations (see Chapter 1).
As program leaders and representatives read this document, they are likely to identify deficits in their programming. This process can be uncomfortable but represents an opportunity for growth and development. Most programs will not manage to fully meet all nine principles. As with medical error reporting and clinical operations improvement in hospital settings, identifying and openly discussing areas for improvement is essential for accountability and progress.
This document was developed collaboratively by a group of veterinarians and researchers from multiple institutions. The original concept was developed at a retreat funded by the Arnall Family Foundation for the Northeast Consortium of Shelter and Community Medicine in 2022. Draft principles were discussed at an open round table at the 2022 Access to Veterinary Care Conference in Minneapolis, Minnesota. The proposed document was then sent to veterinary community engagement experts for comments and review; we deeply appreciate their insight and suggestions. Feedback was discussed and integrated at a follow-up retreat in 2023, also funded by the Arnall Family Foundation. The goal of this document is to enhance understanding of the challenges in designing, implementing, and sustaining veterinary engagement programs and to ensure the dignity, health and welfare of animals and the communities caring for them.
Three appendixes are also included in this document: a glossary of terms (Appendix A), a one-page list of the nine principles (Appendix B), and profiles of veterinary engagement programs (Appendix C). Initiatives selected for inclusion in the program profiles are provided as case examples of individual principles in the document. We are grateful to those who spent time filling out surveys or interviewing with the team about their efforts. Inclusion in this document does not constitute an endorsement of a program. Rather, inclusion is intended to illustrate via example in a different, potentially accessible, way consideration or the use of the principles of veterinary community engagement in a real-life setting.
Finally, a note on language: terminology and concepts change with time, sometimes rapidly. In particular, language describing community relationships and identity are in flux as the world tackles urgent issues in social justice and widespread inequity. We anticipate knowledge and insights will evolve in the field and future findings may contradict parts of what we publish at this time point. We also recognize that terminology cited from the literature may have problematic origins without equivalent replacement terms. As an example, we have used the term ‘interested parties’ throughout this document as a replacement for ‘stakeholders’ due to the covetous connotation of this term, except when citing directly from the primary literature. The language that we use on a daily basis is important and with intention, we can begin to realign historic power imbalances. We ask that our language be taken in the spirit and context that it is intended; these guidelines are presented as a living document and revision will be required.
Chapter 1: Veterinary community engagement: organizing concepts and definitions
Key objective: This chapter provides an abbreviated overview of relevant community engagement definitions and concepts with an emphasis on important and applicable concepts specific to programs that provide animal health services.
Defining community engagement
The Centers for Disease Control and Prevention’s (CDC) Principles of Community Engagement (PCE), which inspired this document, defines community engagement as the process of working collaboratively with groups of people affiliated by geographic proximity, special interest, or similar situations to address issues affecting their well-being. Community engagement is a powerful vehicle for bringing about changes that improve the health of the community and its members.1 In this spirit, we define veterinary community engagement (VCE) as the process of working in collaboration with communities to provide veterinary medical services that impact the health and well-being of animals and humans who care for them. Engagement can take many forms and have different magnitudes (see Fig. 1.1).
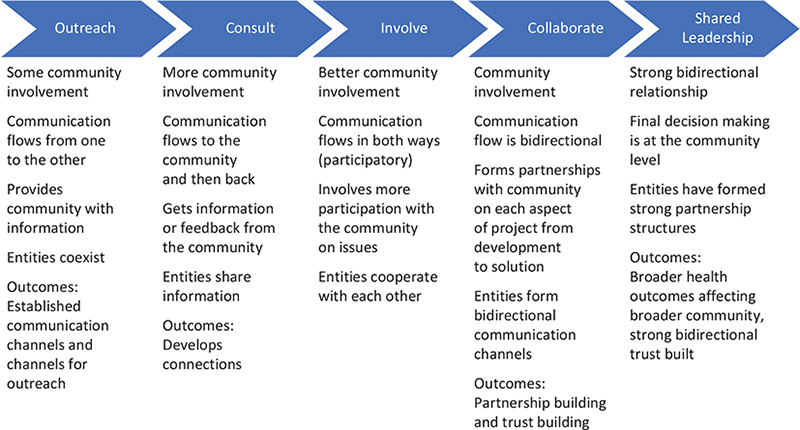
Fig. 1.1. Continuum of community engagement-increasing level of community involvement, impact, trust, and communication flow. Reproduced from CDC.2
Community can be defined in many ways, with relationships representing shared geographic, value-based, and cultural systems while still providing for individual differences. The PCE describes four ‘concepts of community’ which inform community engagement: systems, social, virtual, and individual perspectives.2 These concepts also apply to the process of VCE and interactions with animal owners/caretakers.3
The systems concept views a community as a living creature made of many parts with each component supporting a function essential to the whole.2,4 Organizations and individuals focusing on the care of animals may work alongside or augment human-focused initiatives within a community. A systems approach to community engagement ‘often involves partnerships and coalitions that help mobilize resources and influence systems, change relationships among partners, and serve as catalysts for changing policies, programs, and practices’.1 Applying the systems perspective to the identification of and collaboration between assets in a community increases the impact on animals and people. In addition, as described in the CDC’s Health Equity Guide, prioritization of needs and promotion of health equity within communities should guide the distribution of resources.5
The concept of community can also be viewed through social, virtual, and individual perspectives. Animal owners or caretakers are likely to identify as part of a community or communities not entirely defined by their relationship to animals. The social perspective defines groups within a community by their social and political affiliations. These affiliations can link individuals to other individuals, community organizations and the leaders of those organizations.2 Applying the social perspective of the community to VCE endeavors can help programs identify inconspicuous community leaders through their social ties.
With increasing engagement through technology, the community is not restricted to geographical boundaries. The virtual concept of community also accounts for community through affiliation with groups that exist on social media networks. Individuals may identify as a part of a virtual community based on common interests, including pet ownership.2
The individual conception of community is self-defined and may be based on geography, activities, behaviors, goals for animals (e.g. dog park attendance, virtual pet care forum membership, or community cat colony managers), or as part of a community in which animals serve a particular role (e.g. assistance, emotional support, sports, show, and production). The way in which an animal caretaker views themselves and their animals informs their community identity. For example, animal caretakers may not strongly identify with others around them who own pets (e.g. keeping chickens for food in contrast to keeping backyard pets), which could influence their decision to participate or not participate in programs or opportunities. In many instances, animals and their care activities serve as the conduit for the formation of social support networks and a source of personal identity for those involved.
VCE programs involve many interested parties, including animals, animal caretakers, veterinarians, organizations, governments or individuals who contribute funding or services, community members indirectly impacted by resource allocation or activities, animal sheltering organizations, and students or investigators benefiting from education or research data acquired through the engagement process. Others who do not fall into these categories may also engage with or be impacted by projects in meaningful ways.
Veterinarians employed by animal welfare organizations, commonly identified as shelter veterinarians, are increasingly involved in caring for community animals who belong to clients unable to access and afford veterinary care.6 The expanding mission of animal sheltering organizations, many of whom now provide low-cost services to the public as well as veterinary services for unowned animals such as community cats, reflects a recognition that such populations are potential sources of shelter intake. Thus, the best outcome for many companion animals is to remain in their loving homes and family units, rather than shelter admission or rehoming. These services illustrate the role of the shelter as a public health resource that improves human and animal welfare across communities.
One Health and One Welfare
The mutual relationship between people, animals, and the environment is referred to as One Health.7 One Welfare is defined as the ‘interconnections between animal welfare, human wellbeing and their physical and social environment’.8 The theoretical frameworks that One Welfare utilizes are interdisciplinary, and emphasize the interconnection between animal, human, and environmental health as a critical component of maximizing impact in any one discipline (see Fig. 1.2). A One Welfare approach, in conjunction with the One Health initiative, recognizes the intertwined nature of human, animal, and social welfare, where there has historically been artificial compartmentalization. The health and welfare of companion animals have a direct effect on the health and welfare of their owners, and the community/environment in which they live together.9 The concepts of One Health and One Welfare are a core foundation for discussing and implementing the principles of VCE.
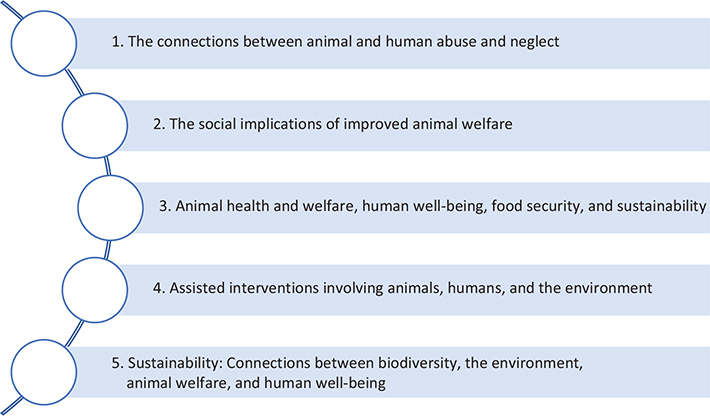
Fig. 1.2. Theoretical frameworks of the One Welfare concept emphasize the interconnections between animal, human, and environmental health to maximize impact across disciplines. Adapted from Pinillos et al.9
Communities benefit when the animals they care for are strong and healthy. Animals provide significant social and health benefits to people.10–12 Animals can also be a source of stress and disease when their caretakers do not have access to basic services, preventive medications, or veterinary care.13 Geographic location, social status, and economic status have significant impacts on human health14; these same factors help determine the health of the animals in communities.15,16 A basic tenet of One Health is that improving environmental and animal well-being also improves human well-being.7
Audience for this document
The intended audience for this document includes individuals engaged in executing and/or participating in community engagement programs which deliver animal health services through a partnership of veterinary professionals and community members. Because animal health services are provided by these programs, it is essential veterinarians are involved in overseeing veterinary care and are engaged in their planning and implementation. However, this resource is not intended only for veterinary use. Other target audiences include university faculty, staff, and students, animal welfare organizations, granting and funding organizations, community partners, and animal shelters engaged in work in their communities, among others.
To help clarify our intentions and align understanding for all audiences, we have included a glossary of terms at the end of this document. At their first use, glossary terms appear with a hyperlink to Appendix A: the glossary.
Scope of this document
Many types of animal-related engagement occur in communities. The scope of this resource is for programs focused on the delivery of animal health services in conjunction with veterinary professionals. Other resources may be more targeted to other types of community engagement activities, such as humane education programs, animal-assisted interventions, and service-animal programs. For example, the International Association of Human-Animal Interaction Organizations (IAHAIO) provides best practices in animal-assisted interventions.17 The Association of Shelter Veterinarians (ASV) offers guidelines specific to animal sheltering organizations, including some guidance about how shelters engage with communities.18 The concepts presented here may also be helpful and relevant to these and other community animal activities.
While it is recognized that VCE occurs internationally, there are limitations to the breadth and depth of what we could include in this resource. Many challenges may exist in the universal application of these principles worldwide, and aspects of the discussion may be most reflective of work performed in the United States (US) by US care providers, due to overrepresentation in this document’s authorship and review. However, international programs may find that this resource can assist in evaluating program design and implementation.
Finally, the authors recognize that policy and advocacy for increased access to animal-related services are essential and necessary within this field and applaud the organizations leading this effort. Guidelines for engaging in advocacy work, both within a community and at a national level, are beyond the scope of this document and are discussed by others.19,20
Ethical frameworks
Ethics in human healthcare has been distilled into three basic principles: beneficence/non-maleficence, which translates most easily into ‘first do no harm’; justice, which means fairness to all, without bias or discrimination; and respect for the person, including respect for the life, autonomy, and dignity of patients.21 Many factors that present ethical and societal challenges in human healthcare are also present in the delivery of clinical care to animals, including health inequities, informed consent, and accessing care.22 Additionally, animals cannot advocate for themselves, provide consent, or exercise autonomy in healthcare choices. Veterinary medicine relies on proxy evaluation of animal welfare to inform recommendations and decision-making. Therefore, it is the responsibility of those engaging in healthcare activities to practice with integrity.23
Fraser’s practical ethic for animals considers One Welfare and One Health concepts and is easily applied in veterinary settings24 (see Table 1.1). This framework focuses on four main principles: providing good lives for the animals in our care, treating suffering with compassion, being mindful of unseen harm, and protecting the life-sustaining processes and balances of nature.25 While this framework was designed for animals, each principle may also be applied to people, communities, and the environment impacted by VCE.
| Ethical Principle | Application of Principles |
| Provide good lives for the animals in our care | A ‘good life’ should be achievable in principle for animals, even if it will require enormous change in practice |
| Treat suffering with compassion | Identify virtues of compassion and mindfulness that should be applied in relevant contexts |
| Be mindful of unseen harm | People who act with compassion and mindfulness should be motivated to avoid and mitigate suffering and unseen harms where they can, while recognizing that some such harms will still exist |
| Protect the life-sustaining processes and balances of nature | This is a call to action in recognition of the great and lasting harm to all inhabitants of the planet which seems likely if action is not taken |
Animal welfare frameworks
The Five Freedoms has informed animal welfare assessments across a wide array of animal-related environments since the late 1960s.26 The Five Domains is an updated reworking of this framework, with an emphasis on increasing positive experiences and recognition of an overall mental state27 (see Table 1.2). In some settings, these frameworks are utilized as a means of evaluating facility or institutional success in animal care. In VCE settings, they are better used to design interventions that support and maintain positive welfare states while also maintaining the human-animal bond present between the animal and the caretaker. Additionally, clinical tools such as pain scales and quality of life assessments can enable treatment decision-making in the context of VCE programs when they are providing individualized clinical services.28–33
| Five Freedoms34 | Five Domains Model for Animal Welfare27 |
| Freedom from hunger and thirst by ready access to water and a diet to maintain health and vigor | Good nutrition, access to fresh water and a diet to maintain health and vigor. Minimize thirst; enable eating to be a pleasurable experience |
| Freedom from discomfort by providing an appropriate environment, including shelter and an appropriate resting area | Good environment; access to shelter, shade, suitable housing, good air quality, and comfortable rest areas. Minimize discomfort, and promote thermal, physical, and other comforts |
| Freedom from pain, injury, and disease by prevention or rapid diagnosis and treatment | Good health: prevention and rapid diagnosis and treatment of disease or injury, fostering good biological functioning. Minimize aversive experiences such as pain and nausea; promote physical activity, vigor, and strength |
| Freedom to express normal behavior by providing sufficient space, proper facilities, and an appropriate company of the animal’s own kind | Appropriate behavior: access to sufficient space, proper facilities, compatible company, and appropriately varied conditions. Minimize threats and unpleasant restrictions on behavior; promote engagement in rewarding activities |
| Freedom from fear and distress by ensuring conditions and treatment which avoid mental suffering | Good feeling (positive mental experiences): access to safe, species-appropriate opportunities to engage in pleasurable activities and experiences. Promote comfort, pleasure, interest, confidence, and a sense of control |
Applying animal welfare and ethical frameworks is essential for individuals and organizations participating in the design, delivery, and evaluation of VCE, to ensure practitioners have considered not only the ethics of caring for an animal but also the priorities and circumstances of humans who represent the animal. The program goal must be an improvement in positive welfare states for both human and animal participants.
Engaging with animal caretakers
To understand whether engagement will be helpful, a VCE activity should begin with a needs assessment. This assessment is a structured inquiry at the level of the community that helps project leaders and community members identify assets and gaps in services or resources in the community.35 In the VCE context, the assessment is focused on animal health services. This process should be performed before a project is started and should center on the perspective of animal caretakers. The people whose animals receive services through community engagement projects require genuine, authentic representation during all phases of the engagement, including inception and design. Representation includes allowing caretakers to act as advocates for their animals, providing input into which services are needed or desired, as well as helping to define project success. Repeat assessments should be performed regularly as a means of program evaluation and recalibration.
Effective and accessible communication is essential to build relationships with animal owners and to identify community goals. The primary languages spoken by those implementing engagement projects and animal owners or caretakers receiving services may be different. In these cases, the inclusion of bilingual personnel is critical since important nuances that deepen understanding between project partners may otherwise be lost. Beyond language, community pet owners and caretakers may have variable access to modes of communication or have different preferences, such as text messaging versus email or phone calls. Choosing the modality that community members can easily access and engage with may need to include recognizing literacy or technological literacy challenges.36
In every project, it is essential to communicate the longevity and scope of services provided to individual project participants. Defining the scope of services that an intervention will or won’t provide is particularly important for clinics with a narrow focus (such as wellness and preventive care); project leaders should be prepared to answer questions and refer owners for care that falls beyond the scope of that engagement (such as care for ill or injured animals). Defining the longevity of the program or how long the community can continue to rely on the project is particularly important for veterinary engagement programs that regularly provide pet food, litter, and other necessities. Owners relying on the project may require additional assistance to locate alternative sources when those provisions become unavailable. Ideally, community engagement projects that provide any kind of service for pet owners include a roadmap for continued community participation and sustainability. Shorter projects ideally operate in the context of larger relationships.
Interdisciplinary collaborations have shown to be very helpful for healthcare, even decreasing errors and improving outcomes.37 Fostering relationships between veterinary and human health providers can be especially helpful when barriers and challenges in interprofessional work are recognized. For example, those engaging in projects involving difficult aspects of pet ownership, such as humane euthanasia or pet hospice care decision-making, generally benefit from including a social worker, especially one trained in the veterinary field.38,39 Social workers can also help veterinarians to understand how a pet impacts their owner’s mental health and distinguish between typical and complicated grief,38 as well as connect individuals to other resources in the community.
Engaging with animals
Animals frequently share the same social determinants of health as their owners, including geographical, economic, and environmental factors.40,41 Animal health projects engaging with communities should be prepared by assessing access to veterinary care (AVC) within the target community, including veterinary care deserts, cost or transportation barriers, and the presence of other engagement projects or community resources, such as shelters or not-for-profit clinics. Projects should be prepared to address the common health concerns faced by animal populations in that location; these concerns may vary between communities, geographical regions, animal species, and populations.
Veterinary interventions provided through community engagement projects are most effective when they follow a spectrum of care or contextualized care model.42–45 Insisting on highly technological and invasive modalities or referrals to tertiary care facilities and specialists because it is perceived as the ‘best care available’ will result in fewer animals being helped and may provide little benefit over more economical or accessible approaches.
There is growing effective care evidence showing lower cost treatment options may be as successful as higher cost options.46,47 The spectrum of care practice emphasizes the importance of collaboration and information exchange between the veterinary team member and animal caretaker, and relies on excellent physical exams, history taking, communication skills, and culturally responsive care (also known as cultural humility, discussed further below).42 Clearly communicating the scope and longevity of the project to community members helps owners select from the care choices available for their animals and understand the limits to care the project can provide.
A least harm approach to effective animal care is recommended. This approach provides care that alleviates distress or suffering even when the medical or behavioral problem may persist, the diagnosis may go unconfirmed, or owner compliance may be uncertain. Some intervention (such as pain medication) is better than not intervening just because optimal care (such as pre-treatment bloodwork) is unavailable. A least harms approach also includes providing only necessary interventions with attention to least intrusive minimally aversive principles.48 For example, requiring a rectal temperature for healthy animals with no history of illness before vaccination is generally unnecessary, increases patient discomfort, may risk staff safety, and prolongs each visit. Full disclosure to owners about the positive and negative implications of different treatment plans should be discussed regardless of income or education level in an accessible way. Choice and autonomy should be provided about how to move forward, even if it involves not utilizing the current clinic options.
Within animal health projects, attention to animal well-being includes close attention to fear, anxiety, and stress (see review by Lloyd).49 Fear Free® Training50 and Low Stress Handling®51 available for veterinary and animal shelter settings are very relevant to VCE activities in other settings. Provisions to decrease pain, stress, and anxiety are important in any project but are particularly critical in VCE projects involving elective surgery. Many economical and effective pain, sedation, and anesthesia protocols are available.52–55 Budgetary constraints do not excuse inadequate pain management in any setting.
Animals impacted by a project do not choose to participate. Owners and caretakers provide consent on behalf of the animals in their care and need to be given all information required for informed consent before participating. Project leaders, educators, and researchers should be subject to and seek official ethical review (e.g. IACUC, IRB, etc.) whenever possible and ensure the positive welfare of animals in teaching or scientific interventions. As part of this review, informed consent for training and/or research and the use of video or images must be obtained. When the VCE project involves oversight by more than one municipality or institution, the project should be subject to whichever ethical norms are the most stringent (see Chapter 6).
The primary goal of all VCE projects should be to enhance the well-being of animals and families in that community. Projects with secondary goals, such as research or education, must also primarily preserve and enhance animal and human welfare. Decisions must be made by project leaders in collaboration with community members that minimize harm and maximize health benefits to individual animals and animal populations.
Engaging with communities
Community-engaged programs succeed when they maintain an asset-based ideology, also known as a strength-based ideology, that emphasizes the strengths or assets of communities and focuses on building relationships.56,57 This approach to community development focuses on what is ‘working’ in the community, instead of only what is ‘not working’, and empowers community members to harness individual and community strengths to enhance whatever services the engagement program might propose.
One of the key assets in a community are proximate leaders. A proximate leader is a part of the community or meaningfully guided by the community’s ideas, agendas, and assets, ‘not just exposed or studying a group of people and its struggles to overcome adversity’.58 Proximate leaders have the relationships, experience, and knowledge to develop approaches with sustainable impact on the community. They also have the ability to identify and leverage community assets that can be ‘overlooked or misunderstood when viewed through a dominant culture lens’.58
Maintaining an asset-based ideology and identifying proximate leaders are key components in counteracting the ‘savior’ mentality/complex in which an outside participant (or organization) perceives their involvement as having an exaggeratedly beneficial impact, and/or that their participation deserves community gratitude. VCE programs that focus on ethical principles and nurturing mutually beneficial relationships naturally become less exploitative and more equitable.
Authentic inquiry regarding the cultural and community beliefs surrounding the husbandry and care of animals, cultural definitions of ‘a good life’ for each species, and the significance of the animals to the local economy is critical. The human-animal bond is often defined as the close, mutually dependent relationship between a caretaker and the animal they are caring for.59 This bond may be valued or structured differently from species to species, culture to culture, or owner to owner. For example, beliefs around animal ‘ownership’, pets living inside the house, or euthanasia, may differ within and between communities.60
Learning about the community’s cultural diversity is part of authentic inquiry. Culturally responsive care and cultural humility training for project participants at all levels is encouraged; inviting members of the community to assist in providing participant orientation is particularly helpful. An understanding that the engagement project represents only a small part of the lived experience of community members helps to counteract the ‘savior’ mentality/complex that can accompany many interventions, both for participants and project leaders.
Within a community, there may be different sub-groups and views. It is important to seek out authentic representation from the project’s community partnerships. In other words, care should be taken to not automatically assume that community-based agencies (such as SPCAs or veterinary clinics) have the same goals as the community members accessing program services. Accessing a community’s social network, defined here as the system of social communication within the community, can help project leadership identify influential community members who may be interested in participating in the project. Creating partnerships with informal or formal community leaders increases impact and allows for more genuine community participation.
Other interested parties
Project partners often have multiple and sometimes competing goals. Projects often include educators, those receiving instruction, and/or researchers, who directly interact with animals and caretakers in the community. Funding agencies, non-governmental or faith-based organizations, and institutions of higher education also may have a vested but indirect interest in the activities and outcomes of VCEs.
Granting organizations, in addition to fulfilling their missions, receive recognition and media coverage.
Grantors and partner organizations, especially universities, should insist on some community orientation or cultural sensitivity training as part of their requirements for funding engagement projects. When services provided to community members are constrained by specific requirements from grantors, these constraints must be communicated to community leaders when designing the projects and individuals seeking services as part of information about the scope of services. Granting organizations should account for the time and effort it takes to develop a program that aligns with community engagement principles in grant timelines and support.
All interested parties gain something from the experience, whether education, field experience, research data, grants, and/or accolades that help advance careers and livelihoods. Both education and discovery are essential to advance the animal welfare field and are frequently the impetus for engagement projects. VCE programs must incorporate an underlying and unequivocal commitment to improving animal welfare. When done properly, these projects thoughtfully provide for community-identified animal needs while supporting experiential learning in animal healthcare and respectful interaction with diverse people.
Transparency and program evaluation
As a component of ethical, transparent practice, all program goals (e.g. education, research, future project plans, fund-raising, and media engagement) should be openly shared with the community and individual animal caretakers prior to initiating the project. Furthermore, to determine whether the project is having the desired effect on the animals and caretakers, every project should include a clear and communicated plan for assessing the project’s interventions and outcomes.
Programmatic evaluation can take many forms, including surveying pet owners, surveying community leaders, or assessing the community’s population of animals for health markers, and can include anthropological, sociological, epidemiological, participatory, or other methodologies. The timing of assessment can be continuous or occur at regular intervals. Projects should not wait until the proposed ‘end’ of the engagement to decide to collect feedback; plans for evaluation should be part of the initial development of any programs or interventions.
Once performed, the results of assessments, whether positive or negative, must be shared with community members in full transparency. When assessment prompts project leaders or community members to consider changes to the project’s original plan or scope, these changes should be proposed and agreed upon by all affected parties. A plan for further assessment should be made at that time (see Chapter 6).
References
| 1. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. CDC/ATSDR Committee on Community Engagement. 1st ed. 1997. |
| 2. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 3. | Wood L, Martin K, Christian H, et al. The pet factor – companion animals as a conduit for getting to know people, friendship formation and social support. PLoS One. 2015;10(4):e0122085. doi: 10.1371/journal.pone.0122085 |
| 4. | Thompson B, Kinne S. Chapter 2: Social change theory: applications to community health. In: Bracht N, ed. Health Promotion at the Community Level: New Advances. Sage Publications. 2nd ed. 1998:29–28. |
| 5. | Centers for Disease Control and Prevention – Division of Community Health. A Practitioner’s Guide for Advancing Health Equity: Community Strategies for Preventing Chronic Disease. US Department of Health and Human Services; 2013. |
| 6. | Shelter Animals Count. Community Services Data. 2022. https://www.shelteranimalscount.org/community-services-data-report-2022. Accessed May 24, 2024. |
| 7. | Centers for Disease Control and Prevention (CDC). One Health. https://www.cdc.gov/onehealth/index.html. Accessed April 14, 2023. |
| 8. | One Welfare. About One Welfare. https://www.onewelfareworld.org/. Accessed April 13, 2023. |
| 9. | Pinillos RG, Appleby MC, Manteca X, Scott-Park F, Smith C, Velarde A. One welfare – a platform for improving human and animal welfare. Vet Record. 2016;179(16):412–413. doi: 10.1136/vr.i5470 |
| 10. | Christian HE, Westgarth C, Bauman A, et al. Dog ownership and physical activity: a review of the evidence. J Phys Act Health. 2013;10(5):750–759. doi: 10.1123/jpah.10.5.750 |
| 11. | Levine GN, Allen K, Braun LT, et al. Pet ownership and cardiovascular risk: a scientific statement from the American Heart Association. Circulation. 2013;127(23):2353–2363. doi: 10.1161/CIR.0b013e31829201e1 |
| 12. | McConnell AR, Brown CM, Shoda TM, Stayton LE, Martin CE. Friends with benefits: on the positive consequences of pet ownership. J Personal Soc Psychol. 2011;101(6):1239. doi: 10.1037/a0024506 |
| 13. | LaVallee E, Mueller MK, McCobb E. A systematic review of the literature addressing veterinary care for underserved communities. J Appl Animal Welfare Sci. 2017;20(4):381–394. doi: 10.1080/10888705.2017.1337515 |
| 14. | Marmot M. Social determinants of health inequalities. Lancet. 2005;365(9464):1099–1104. doi: 10.1016/S0140-6736(05)71146-6 |
| 15. | McDowall S, Hazel SJ, Chittleborough C, Hamilton-Bruce A, Stuckey R, Howell TJ. The impact of the social determinants of human health on companion animal welfare. Animals. 2023;13(6):1113. doi: 10.3390/ani13061113 |
| 16. | Neal SM, Greenberg MJ. Putting access to veterinary care on the map: a veterinary care accessibility index. Front Vet Sci. 2022;9:219. doi: 10.3389/fvets.2022.857644 |
| 17. | International Association of Human-Animal Interaction Organizations (IAHAIO). The IAHAIO definitions for animal assisted intervention and guidelines for wellness of animals involved in AAI [white paper]. 2018. https://iahaio.org/best-practice/white-paper-on-animal-assisted-interventions/. Accessed August 24, 2023. |
| 18. | The Association of Shelter Veterinarians (ASV). The guidelines for standards of care in animal shelters: second edition. J Shelter Med Commun Anim Health. 2022;1:1–76. doi: 10.56771/ASVguidelines.2022 |
| 19. | American Public Health Association. Top Ten Rules of Advocacy. https://www.apha.org/policies-and-advocacy/advocacy-for-public-health/coming-to-dc/top-ten-rules-of-advocacy#:~:text=Be%20brief%2C%20cle. Accessed August 14, 2023. |
| 20. | Golden SD, McLeroy KR, Green LW, Earp JAL, Lieberman LD. Upending the Social Ecological Model to Guide Health Promotion Efforts Toward Policy and Environmental Change. Los Angeles, CA: Sage Publications; 2015:8S–14S. |
| 21. | Beauchamp TL, Childress JF. Principles of Biomedical Ethics. Oxford University Press; 1979. |
| 22. | National Council for Mental Wellbeing. Addressing Health Equity and Racial Justice within Integrated Care Settings. https://www.thenationalcouncil.org/resources/integrated-health-coe-toolkit-purpose-of-this-toolkit/. Accessed August 14, 2023. |
| 23. | Grimm H, Bergadano A, Musk GC, Otto K, Taylor PM, Duncan JC. Drawing the line in clinical treatment of companion animals: recommendations from an ethics working party. Vet Record. 2018;182(23):664. doi: 10.1136/vr.104559 |
| 24. | Fawcett A, Mullan S, McGreevy P. Application of Fraser’s ‘practical’ ethic in veterinary practice, and its compatibility with a ‘one welfare’ framework. Animals. 2018;8(7):109. doi: 10.3390/ani8070109 |
| 25. | Fraser D. A ‘practical’ ethic for animals. J Agri Environ Ethics. 2012;25:721–746. doi: 10.1007/s10806-011-9353-z |
| 26. | Brambell F. Report of the Technical Committee to Enquire into the Welfare of Livestock Kept under Intensive Conditions. Her Majesty’s Stationery Office; 1965. |
| 27. | Mellor DJ, Beausoleil NJ, Littlewood KE, et al. The 2020 five domains model: including human–animal interactions in assessments of animal welfare. Animals. 2020;10(10):1870. doi: 10.3390/ani10101870 |
| 28. | Costa R, Hassur R, Jones T, Stein A. The use of pain scales in small animal veterinary practices in the USA. J Small Animal Pract. 2023;64(4):265–269. doi: 10.1111/jsap.13581 |
| 29. | Evangelista MC, Watanabe R, Leung VS, et al. Facial expressions of pain in cats: the development and validation of a Feline Grimace Scale. Sci Rep. 2019;9(1):19128. doi: 10.1038/s41598-019-55693-8 |
| 30. | Gardner M. Quality of life assessment and end of life decisions. In: Gardner M, McVety D, eds. Treatment and Care of the Geriatric Veterinary Patient. Wiley Blackwell/John Wiley & Sons Inc.; 2017:297–310. |
| 31. | Mullan S. Assessment of quality of life in veterinary practice: developing tools for companion animal carers and veterinarians. Vet Med. 2015;6:203–210. doi: 10.2147/VMRR.S62079 |
| 32. | Oyama MA, Citron L, Shults J, Cimino Brown D, Serpell JA, Farrar JT. Measuring quality of life in owners of companion dogs: development and validation of a dog owner-specific quality of life questionnaire. Anthrozoös. 2017;30(1):61–75. doi: 10.1080/08927936.2016.1228774 |
| 33. | Yeates J, Main D. Assessment of companion animal quality of life in veterinary practice and research. J Small Animal Pract. 2009;50(6):274–281. doi: 10.1111/j.1748-5827.2009.00755.x |
| 34. | Farm Animal Welfare Council. Farm Animal Welfare in Great BritaIn: Past, Present and Future. Department for Environment, Food & Rural Affairs; 2009. |
| 35. | Centers for Disease Control and Prevention (CDC). Community Needs Assessment. https://www.cdc.gov/globalhealth/healthprotection/fetp/training_modules/15/community-needs_pw_final_9252013.pdf. Accessed April 14, 2023. |
| 36. | Centers for Disease Control and Prevention (CDC). Inclusive Communication Principles. https://www.cdc.gov/healthcommunication/Health_Equity.html. Accessed August 14, 2023. |
| 37. | Fewster-Thuente L, Velsor-Friedrich B. Interdisciplinary collaboration for healthcare professionals. Nurs Admin Quarter. 2008;32(1):40–48. doi: 10.1097/01.NAQ.0000305946.31193.61 |
| 38. | Holcombe TM, Strand EB, Nugent WR, Ng ZY. Veterinary social work: practice within veterinary settings. J Hum Behav Soc Environ. 2016;26(1):69–80. doi: 10.1080/10911359.2015.1059170 |
| 39. | Hoy-Gerlach J, Ojha M, Arkow P. Social workers in animal shelters: a strategy toward reducing occupational stress among animal shelter workers. Front Vet Sci. 2021;8:734396. doi: 10.3389/fvets.2021.734396 |
| 40. | Card C, Epp T, Lem M. Exploring the social determinants of animal health. J Vet Med Educ. 2018;45(4): 437–447. doi: 10.3138/jvme.0317-047r |
| 41. | Patronek GJ. Mapping and measuring disparities in welfare for cats across neighborhoods in a large US city. Am J Vet Res. 2010;71(2):161–168. doi: 10.2460/ajvr.71.2.161 |
| 42. | Brown CR, Garrett LD, Gilles WK, et al. Spectrum of care: more than treatment options. J Am Vet Med Assoc. 2021;259(7):712–717. doi: 10.2460/javma.259.7.712 |
| 43. | Fingland RB, Stone LR, Read EK, Moore RM. Preparing veterinary students for excellence in general practice: building confidence and competence by focusing on spectrum of care. J Am Vet Med Assoc. 2021;259(5):463–470. doi: 10.2460/javma.259.5.463 |
| 44. | Skipper A, Gray C, Serlin R, O’Neill D, Elwood C, Davidson J. ‘Gold standard care’ is an unhelpful term. Vet Record. 2021;189(8):331. doi: 10.1002/vetr.1113 |
| 45. | Stull JW, Shelby JA, Bonnett BN, et al. Barriers and next steps to providing a spectrum of effective health care to companion animals. J Am Vet Med Assoc. 2018;253(11):1386–1389. doi: 10.2460/javma.253.11.1386 |
| 46. | McCobb E, Dowling-Guyer S, Pailler S, Intarapanich NP, Rozanski EA. Surgery in a veterinary outpatient community medicine setting has a good outcome for dogs with pyometra. J Am Vet Med Assoc. 2022;260(S2):S36–S41. doi: 10.2460/javma.21.06.0320 |
| 47. | Perley K, Burns CC, Maguire C, et al. Retrospective evaluation of outpatient canine parvovirus treatment in a shelter-based low-cost urban clinic. J Vet Emerg Crit Care. 2020;30(2):202–208. doi: 10.1111/vec.12941 |
| 48. | The Association of Professional Dog Trainers (APDT). Position Statement on LIMA. https://apdt.com/wp-content/uploads/2017/01/position-statement-lima.pdf. Accessed April 13, 2023. |
| 49. | Lloyd JKF. Minimising stress for patients in the veterinary hospital: why it is important and what can be done about it. Vet Sci. 2017;4(2):22. doi: 10.3390/vetsci4020022 |
| 50. | Fear Free. Fear Free Shelters. 2023. https://fearfreeshelters.com/. Accessed April 6, 2023. |
| 51. | Cattle Dog Publishing. What Is Low Stress Handling? https://cattledogpublishing.com/why-and-what-is-low-stress-handling/. Accessed April 13, 2023. |
| 52. | Costa RS, Karas AZ, Borns-Weil S. Chill Protocol to Manage Aggressive & Fearful Dogs. https://digital.cliniciansbrief.com/digital-edition/clinicians-brief-may-2019#48592. Accessed April 13, 2023. |
| 53. | Griffin B, Bushby PA, McCobb E, et al. The association of shelter veterinarians’ 2016 veterinary medical care guidelines for spay-neuter programs. J Am Vet Med Assoc. 2016;249(2):165–188. doi: 10.2460/javma.249.2.165 |
| 54. | Ko JC, Berman AG. Anesthesia in shelter medicine. Topics Compan Animal Med. 2010;25(2):92–97. doi: 10.1053/j.tcam.2010.03.001 |
| 55. | The Humane Society of the United States (HSUS). Spayathon for Puerto Rico. 2019. https://maddiesmillionpetchallenge.org/wp-content/uploads/Spayathon-Information-Packet.pdf. Accessed May 24, 2024. |
| 56. | Blickem C, Dawson S, Kirk S, et al. What is asset-based community development and how might it improve the health of people with long-term conditions? A realist synthesis. SAGE Open. 2018;8(3):215824401878722. doi: 10.1177/215824401878722 |
| 57. | Kretzmann J, McKnight J. Building Communities from the Inside Out: A Path toward Finding and Mobilizing a Community’s Assets. ACTA Publications; 1993. |
| 58. | Jackson A, Kania J, Montgomery T. Effective change requires proximate leaders. Stanford Soc Innov Rev. 2020. https://doi.org/10.48558/DBNF-V067. |
| 59. | Fine AH. Handbook on Animal-Assisted Therapy: Theoretical Foundations and Guidelines for Practice. 3rd ed. Elsevier Academic Press; 2010. |
| 60. | Elmore RG. The lack of racial diversity in veterinary medicine. J Am Vet Med Assoc. 2002;222(1):24–26. doi: 10.2460/javma.2003.222.24 |
Chapter 2: Principles of veterinary community engagement
*Adapted from Principles of Community Engagement 2nd edition1
Key objective: This chapter outlines nine pillars of veterinary community engagement (VCE) (Fig. 2.1), modeled after the Centers for Disease Control and Prevention’s (CDC) Principles of Community Engagement (PCE) for human health.1
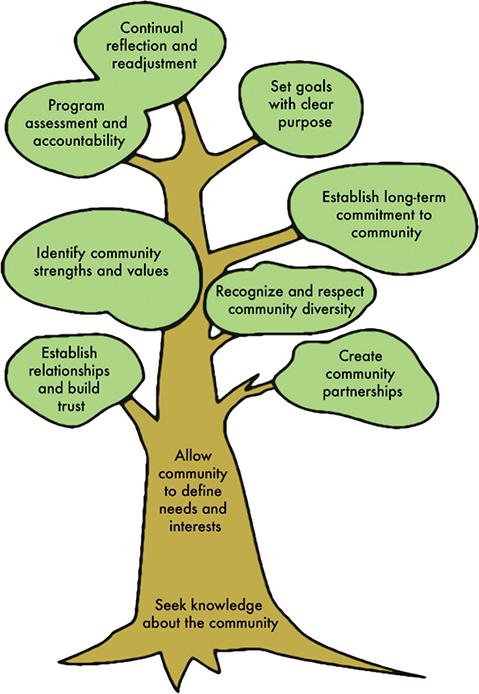
Fig. 2.1. Visual diagram of nine pillars of veterinary community engagement, modeled after the CDC’s principles of community engagement for human health.1
Introduction
Veterinary engagement in communities with limited access to care is vital for the health and wellness of both animals and humans. Even well-intentioned programs can have negative impacts on individuals and communities. Thoughtful and intentional engagement practices are needed to ensure ethical and sustainable community initiatives. Building trust and creating lasting relationships with community members, as well as community organizations, is fundamental for program success.
In the United States, veterinary practices have generally been located in white, affluent communities, with about 93% of veterinary doctors identifying as white.2 Historically, the veterinary medical industry has poorly supported inclusivity in animal ownership, instead focusing on the care of pets of owners with means to access care and largely ignoring those that could not.3,4 Likewise, animal control and welfare efforts in marginalized communities in the United States have frequently focused on animal seizure and surrender rather than owner engagement.5,6 For both fields, these practices have resulted in the promotion of attitudes of superiority/inferiority and created barriers to trust with people caring for animals in underserved communities. As a result, communities may be reluctant to engage with entities that remind some of their members of previous poor experiences. It is essential to increase access to veterinary care (AVC) in diverse communities, as well as increase diversity in the veterinary profession.
In order to promote equitable relationships and prevent barriers to trust, we offer these nine principles or pillars of VCE modeled on the Principles of Community Engagement.1 Although these pillars are numbered, they are not intended to be followed in a linear approach. In fact, the activities discussed in the principles should occur simultaneously and repeatedly throughout the process of developing, implementing, assessing, and continually renewing a VCE project.
Principle 1
‘Become knowledgeable about the community’s culture, economic conditions, social networks, political and power structures, norms and values, demographic trends, history, and experience with efforts by outside groups to engage… Learn about the community’s perceptions of those initiating the engagement activities’.1
Using both qualitative and quantitative measures, authentic inquiry should be employed to learn as much as possible about a community – including how they perceive their pets – to foster a successful partnership between an organization and a community. Additionally, VCE leaders should seek to understand how the community perceives the benefits and costs of participating in the project, in order to address misconceptions and concerns from the beginning.
Principle 2
‘Go to the community, establish relationships and build trust, work with the formal and informal leadership, and seek commitment from community organizations and leaders to create processes for mobilizing the community’ in an ethical and evidence-based way.1
Similar to community engagement in human healthcare, programs succeed and grow when members of the community are active partners in their planning and implementation. This process requires fostering relationships built on trust and mutual respect between an organization or individual and the community’s interested parties. There are many actions, from meeting at a location within the community to identifying multiple interested parties to include in the planning process, that signal and facilitate the establishment of a solid working relationship. Other examples include the provision of appropriate, close supervision of trainees and post-operative support for complications resulting from student learning in VCE clinical settings. An approach which takes into account the animal, caretaker, and evidence-based contextualized care and high ethical principles should be employed to provide optimal client and patient welfare.
Principle 3
Partner with the community to create change and improve community health and animal welfare.1 Recognize how, as a program leader and care provider, your identity influences this partnership.
Partnership implies mutual respect, reciprocity, and investment in meeting collectively established goals. Members of the community must be active and respected participants in the project. Veterinarians, for example, should recognize the power inherent in their role, as well as how their past experiences, identity and personal values may impact their perspective. Ideally, veterinarians work with partners to coordinate the expected healthcare activities, generate ideas, and understand community initiatives from the beginning. Organizations need the flexibility to listen and adapt to community feedback. Community needs assessments in partnership should identify both needs and assets that exist in that community and recognize the community’s strengths as well as its challenges. Power dynamics between outside organizations and community members are often disproportionate; therefore, it is crucial to work equitably and acknowledge any power differentials that may impact relationships.
Principle 4
‘Remember and accept that collective self-determination is the responsibility and right of all people in a community. No external entity should assume it can bestow on a community the power to act in its own self-interest’”.1 Organizations that wish to engage a community as well as individuals seeking to effect change must be prepared to release control of actions or interventions to the community and be flexible to meet its changing needs.
Maintaining an asset-based, community driven approach while engaging with communities leads to equitable and sustainable relationships. The ‘savior’ mentality or organizational overreach leads to community disengagement and inequitable power imbalances. Autonomy of community members to make decisions that align with their cultural/ethical priorities is essential to building a strong relationship. For example, while requiring animals to be spayed or neutered in order to receive low-cost urgent care may help an organization meet their mission to decrease pet overpopulation, it may also jeopardize engagement by removing owner agency and participation, compromising community and animal care.
Principle 5
All aspects of community engagement must be designed to recognize and respect diversity within the community and the partnership. Acknowledge how identity impacts planning, design, and implementation.1
The diversity of a community is recognized in many variables, from socioeconomic status to shared culture and history, and more. Recognition of the ways in which community members differ plays a major role in how participants engage. For example, language is a common barrier to accessible veterinary care. A project in a community where many languages are spoken will need to ensure that verbal or written communication is not a barrier to care access for any subset of the community.
Principle 6
Be clear and transparent about the purpose or goals of the community engagement project and recognize that interested parties will come to a partnership with equally important but different goals.1
Representatives of the partner community should be actively engaged in goal setting and defining priorities. All participating individuals and organizations should be able to articulate why they wish to be involved. The impetus for veterinary engagement is less often the result of a legislative change and more often the result of organizations wishing to expand or fulfill their mission in a different fashion. Examples might include a non-profit organization which received a grant to provide vaccinations or a veterinary school that wishes to improve the hands-on training their students receive. VCE projects benefit from clear goals and an agreed upon scope of services, such as a vaccine clinic to reduce infectious disease incidence in the community or a community clinic to improve access to veterinary care or animal care in general. As discussed in the CDC’s PCE document for human healthcare settings,7 a narrower focus leads to a more easily managed project while a broader focus can lead to a greater impact within the community as a whole.
Principle 7
‘Community engagement can only be sustained by identifying and mobilizing community assets and strengths and by developing the community’s capacity and resources to make decisions and take action’.1
Every community has specific assets, strengths, and resources, as well as concerns and challenges highlighted by passionate individuals and organizational advocates. VCE projects wishing to develop sustainable community initiatives should harness community strengths and assets, and foster community growth and development. For example, partnering with a transportation business based in the community to provide rides to a clinic for owners and their pets both harnesses a community-based strength and promotes its growth. A community-based pet food pantry with a solid base in development may be able to take ownership of the solicitation of potential donors and collection of donations from external organizations.
Principle 8
Community collaboration requires a long-term commitment to have the best chance at a measurable and sustainable impact.1
Many veterinary engagement initiatives begin with a specific funding opportunity which may only enable the execution of a single event. However, the health and care of animals are best served when community collaboration occurs over time and with an eye to sustained efforts and relationships. Successful partnerships are built on a foundation of trust and mutual respect; new partnerships take time to establish and in general, programs are more effectively planned with a commitment to sustainability, not in reaction to short-term funding availability. Funding organizations are specifically encouraged to commit support over periods more conducive to authentic partnerships (e.g. years or multiple years) and to promote VCE projects in line with these principles. Any events or projects intended on a shorter timeline should be part of a larger relationship or commitment to the community itself.
Principle 9
Successful community collaboration requires continual reflection, both individually and as a group. Accountability and assessment of VCE programming is crucial for continued success.
Collaborators should take time to establish the definition of a ‘successful program’ in the eyes of all interested parties, recognizing priorities may differ. Identifying the criteria, concerns, and limitations prior to starting a program is ideal. Assessment of community engagement requires both individual and organizational reflection at multiple time-points. For individuals, recognizing internal bias and judgment is crucial to growth and fostering connection. Additionally, structured reflection is essential to building skills in interpersonal communication, problem solving, self-awareness, and a sense of civic responsibility. In particular, as healthcare providers, veterinarians are encouraged to reflect on their role in the face of increasingly complex challenges in access to care for communities. Program-level reflection includes evaluation of data to assess impact and shape evolution of the project. Sharing and connecting with others about experiences, successes, and failures supports continued learning within and outside of the community and can improve community engagement programming on a much larger scale.
In conclusion, sustainable community engagement efforts are fostered through shared connections, relationship building and deep listening. Veterinarians and other animal healthcare professionals experience burnout and moral distress at a higher rate than other professions.8–12 By nature, VCE programs that are delivering medical care rely on these professional providers. It is important for all participants to routinely connect with partners and peers about goals, expectations, successes, and challenges to promote long-term sustainable relationships.
Applying these pillars will aid in the process of VCE by centering the voices and lived experiences of animal caretakers and other interested parties in the community. If missteps or mistakes are made, leaders should acknowledge responsibility and maintain open communication to find mutually beneficial solutions. Recognizing and reflecting on internal bias, as well as the impacts of institutional and structural privilege and racism, is a lifelong process.
References
| 1. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 2. | U.S. Bureau of Labor Statistics. Labor Force Characteristics by Race and Ethnicity. 2019. https://www.bls.gov/opub/reports/race-and-ethnicity/2019/home.htm. Accessed April 7, 2023. |
| 3. | LaVallee E, Mueller MK, McCobb E. A systematic review of the literature addressing veterinary care for underserved communities. J Appl Animal Welfare Sci. 2017;20(4):381–394. doi: 10.1080/10888705.2017.1337515 |
| 4. | The Humane Society of the United States (HSUS). Pets for Life – A New Community Understanding. https://www.humanesociety.org/sites/default/files/docs/2012-pets-for-life-report.pdf. Accessed April 14, 2023. |
| 5. | Hawes SM, Hupe T, Morris KN. Punishment to support: the need to align animal control enforcement with the human social justice movement. Animals. 2020;10(10):1902. doi: 10.3390/ani10101902 |
| 6. | Marceau J. Beyond Cages: Animal Law and Criminal Punishment. Cambridge University Press; 2019. |
| 7. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 1st ed. 1997. |
| 8. | Andrukonis A, Protopopova A. Occupational health of animal shelter employees by live release rate, shelter type, and euthanasia-related decision. Anthrozoös. 2020;33(1):119–131. doi: 10.1080/08927936.2020.1694316 |
| 9. | Merck Animal Health. Merck Animal Health Veterinary Wellbeing Study III. https://www.merck-animal-health-usa.com/about-us/veterinary-wellbeing-study. Accessed August 24, 2023. |
| 10. | Neill CL, Hansen CR, Salois M. The economic cost of burnout in veterinary medicine. Front Vet Sci. 2022;9:814104. doi: 10.3389/fvets.2022.814104 |
| 11. | The Association of Shelter Veterinarians (ASV). ASV Member Survey Reveals Profound Concern with Shelter Veterinarian Retention and Offers a Glimpse into Solutions. https://www.sheltervet.org/assets/PDFs/Survey%20Results%20and%20Member%20Discussion%20Summary.pdf. Accessed April 13, 2023. |
| 12. | Tomasi SE, Fechter-Leggett ED, Edwards NT, Reddish AD, Crosby AE, Nett RJ. Suicide among veterinarians in the United States from 1979 through 2015. J Am Vet Med Assoc. 2019;254(1):104–112. doi: 10.2460/javma.254.1.104 |
Chapter 3: Ethical considerations for veterinary community engagement
Key objective: This chapter outlines core ethical considerations for veterinary community engagement (VCE), including an emphasis on training programs.
Introduction
There is increased recognition among academic institutions and large non-profit organizations of the many benefits of VCE for applied training opportunities for veterinary professionals and increasing access to care. Robust opportunities are available but many fail to recognize the complexity of creating authentic partnerships or to subscribe to foundational animal welfare and ethical frameworks. Integrating these nine pillars into the program design, training opportunities, and interpersonal interactions with community leadership and individuals is a complicated process that takes time and thought. The ultimate goal is that all participants are in a better place than when they came to the partnership.
Program oversight
VCE programs must utilize qualified animal healthcare providers who have relevant licensure and are familiar with the legal restrictions for veterinary practice. In some programs, provision of medical advice may be provided through paraprofessionals or lay people; however, the program should have written protocols and consistent oversight by a veterinarian who has approved this provision of care, and who is available for consultation, questions, or follow-up. This model of veterinary oversight is commonly practiced in population settings such as animal shelters to optimize efficient high-quality care delivery.1 In addition to providing and documenting medical records, programs must identify and adhere to local, regional, and national laws beyond those directly related to veterinary services.
Program design
Cultural humility
Developing cultural humility is more than a recognition that one group may be different from another or from the prevailing norm in the region or community. It is common to attribute differences to cultural, moral, or ethical factors, but community conditions are determined by economic, social, and political factors as much as behaviors and beliefs.2,3 Acknowledging how historical power and privilege have shaped communities and informed community-engaged partnerships is essential to all engaged work (Principle 5). It is especially important when considering the history of academic work or research in communities with fewer resources.4,5
Caregiving and decision-making
In addition to the ethical and welfare frameworks presented in Chapter 1, VCE program design must be based on principles of empowerment of individuals and communities to play an active role in defining goals of the program and the interactions and the care provided to patients (Principle 6). Animal caretakers must be involved in decision-making at all levels and points in time. Every act is a collaboration which recognizes the value of all participants and recognizes that no single entity can accomplish what they are able to do together.
In human medicine, an emphasis on patient and family-centered care has shifted the focus from the physician as the provider to the patient and family unit to a model in which patients and families partner with the physician in attaining successful healthcare outcomes.6 This shift in focus is relevant in many veterinary contexts. A Family Quality of Life (FQoL) approach to veterinary clinical decision-making takes family-centric, patient-centric, and external factors all into account.7 The FQoL approach is particularly applicable in the community-engaged clinic context, where the animal caretaker may take a more active role in the provision of care at home due to resource limitations or patient/client preferences. An adapted diagram for veterinary contexts is shown in Fig. 3.1.

Fig. 3.1. Diagram adapted from Catalyst8 describing the concept of patient and client-centered care as it relates to veterinary medicine and clinical decision-making.
Scope of the work
Programs should consciously define the scope and capacity of the program to do compassionate work that reflects animal welfare principles (Principle 6). Optimal outcomes include a broad spectrum of treatment options and educational opportunities; animal welfare should be central to this decision-making process and take into account all aspects of patient management, including post-operative care and follow-up.
In addition to providing evidence-based contextualized care, programs should aim to provide positive experiences for human and animal participants in the context of a clinical interaction. Examples include incorporating positive reinforcement techniques in animal handling, providing appropriate medical services for diagnosed conditions, and ensuring nutritional support adequate for life-stages or other needs.9,10
Provision of care relies on the investment of resources by the family unit as well as the clinical program (Principle 3). Clinical decision-making should always involve a clear understanding of the level of investment required of all interested parties (see Fig. 3.2). There should be clear criteria for what an optimal outcome looks like for each party. An overall outcome that might seem ‘good enough’ for the clinician in the context of a training program or constrained resources might not adequately meet the overall welfare needs of the animal or the caretaker or the community as a whole.
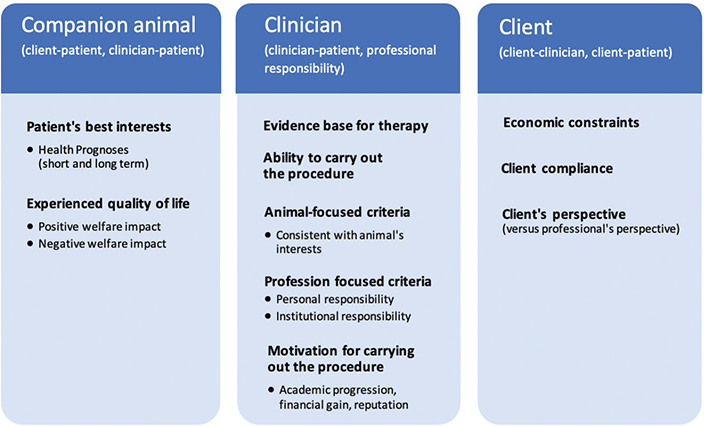
Fig. 3.2. Diagram showing the key interested parties, relationship domains, and criteria to be considered in veterinary ethical decision-making. Adapted from Grimm et al.11
Events and the scope of programming must be coordinated with partner organizations already acting in the community to be considered engaged work. This coordination prevents overlapping of services and creates synergy and efficiency between engaged organizations and the community they serve. Providing services in a location without a consistent veterinary presence does not necessitate a decreased quality of care or a lack of protocols. In fact, well-structured and supervised care by trained animal care staff and trainees can often accomplish highly effective care.
Client recruitment and engagement
Selection of participants in programs should not default to those most available or convenient for medical care providers. Programs should also be designed to protect human and animal participants from needing to expend efforts or expenses beyond what is a reasonable expectation of a community member. This goal is accomplished by ensuring that animal caretakers have access to information and program support at all steps of the process.
Similarly, participants should not be put at undue risk to meet the needs of programming. For example, it is not appropriate to expose humans who may be particularly vulnerable to infectious disease to large numbers of volunteers, especially if appropriate personal protective equipment, hand hygiene, or physical distancing is not available. Likewise, congregating large numbers of people and animals in a small space or unsafe area may increase the likelihood of anxiety or injury.
Promotional work and use of media
The use of media and public relations should be considered carefully. Promotional descriptions of these activities, as with all community work, should accurately reflect the goals and impact; for example, a program performing 20 animal surgeries per year while training students does not impact overpopulation and therefore should not be marketed as such.
Building an understanding of a program among external interested parties and the public often relies on sharing stories and experiences and can be critical to long-term operations and funding. When implemented correctly, sharing stories can also engage populations accessing services in a meaningful way and can be empowering, as noted in some storytelling efforts in groups like veterans’ groups.12 Organizations should provide care and training regardless of whether the participants are willing to be identified publicly; sometimes being identified publicly can put individuals at risk.
Consent
Informed consent should be freely given. Participants should not be required to consent to all recommendations in order to access some components of services. Programs should provide clear releases, accommodations, and communication outlets for concerns. See Chapter 6 for more discussion on research-focused informed consent.
Recordkeeping
All programs must keep complete medical records in keeping with regulatory requirements for veterinary practice, including controlled drug disposition. Medical records should be made available to owners and veterinary professionals upon request; copies of medical information and care instructions must be provided to pet owners receiving services.
Follow-up care
Accessible care services are often most needed in communities which experience barriers to urgent care and emergency services. A plan and resources should be available to help caretakers access emergency care when complications arise after wellness or spay-neuter clinics. This follow-up care is particularly important if trainees are involved in providing services, since complication rates, or the perception of increased complications, may be higher.13 Likewise, when initiatives take place outside of a clinic or hospital environment, a plan should be in place for accessing such care in the rare event it becomes necessary. There may also be legal and/or professional obligations to provide a pathway for follow-up care; regardless, there is a moral and practical obligation to do so.
Reflection activities following events
Post-event reflections and debrief exercises should be integrated into program design. These types of exercises encourage meaningful reflection and information gathering and capture the experience of the volunteers, staff, and trainees involved. Reflections can elucidate prejudices or conflicts and improve practices. They can also provide avenues for further learning or, in the event that mentally distressing experiences are encountered, provide a way to connect participants to support services. Continual self-evaluation can help combat issues such as ‘savior’ mentality/complex that can be seen in international and academic work.14
Ongoing collaborations
Longitudinal work is more effective at solving long-term, systemic issues of access to veterinary care (AVC) and at providing comprehensive training programs (Principle 8). One-time events can pose significant challenges to building trust and creating sustainable outcomes and partnerships. For example, single outreach events affiliated with meetings or conferences may offer an interesting service opportunity to visitors but likely have limited utility in addressing community need, unless it is temporarily supporting a core program maintained in the community.
Ethical considerations in the use of volunteer labor in community engagement
Core to the pillars of VCE are relationship building, trust, and mutual respect in partnerships. These relationships can be difficult to establish with a high level of personnel turnover, including a reliance on temporary volunteers to accomplish programming. The use of volunteer labor in VCE programs has the potential to encounter some common pitfalls if the program is not structured to account for these issues. At the same time, volunteering is often an entry point for participants to become more active in solving what are widespread systemic issues.15 Indeed, volunteers are the backbone of many programs practicing VCE.
Animal welfare as an industry has a long history of relying on volunteerism and philanthropy. A traditional philanthropy approach relies on people of privilege to accomplish the work through their ‘acts of kindness’. This approach risks being culturally insensitive (Principle 2) and inequitable and fails to examine the systemic issues creating the underlying inequities that community engagement should be addressing. It also, by default, excludes individuals without the financial means to volunteer. One consequence is that animal welfare as an industry has failed to adequately include or represent lower income and BIPOC communities, and this has been identified as a critical issue needing further investigation.16,17
Programs should evaluate whether heavy reliance on volunteers has the potential to negatively impact opportunities for veterinary experiences for members of lower income and BIPOC communities because dominant groups in society are more likely to be able to volunteer.18 Many aspects of programming may be better accomplished by creating paid, stable positions hired within the community. Investing in proximate leaders and core staff from the community supports long-term, integrative partnerships.19
This disparity among those who can afford to volunteer can be particularly poignant when considering applicants to veterinary colleges. Acceptance to veterinary training programs generally requires a significant number of hours of clinical experience, which are often attained through volunteering.20 This requirement may be unattainable as an unpaid experience for lower income candidates when volunteerism is considered the model.
In some situations, volunteers may be inexperienced or struggle with elements of their assignments; examples include deficiencies in cultural and clinical communication, clinical knowledge, cultural humility, safe animal handling, and other essential skills. To mitigate this risk, volunteer training requirements should be rigorous and completed prior to events, and participants should demonstrate specific competencies prior to participation in an activity.
To volunteer is to assume a position of privilege. While volunteers are necessary for many programs to adequately staff events, relying on volunteers can compromise the sustainability and impact of the program in the community. Community engagement, practiced as an authentic partnership, is a professional activity informed by medical practice, social work, ethical frameworks, and regulatory matters. VCE requires careful, intentional, and thoughtful planning in the development, execution, and assessment of efforts to ensure authentic attention to human and animal welfare. There is an ethical necessity for reflective practice even when participating as a volunteer.
Training programs
Foundational ethical and animal welfare principles must remain intact even with the added challenges of training contexts. Although many training programs are primarily focused on the provision of medical services, additional welfare needs must be considered when designing a training program (see Table 1.2). Community members should be fully informed of and consent to the involvement and roles of students in community work.
By its nature, teaching means processes take longer than those carried out by qualified and experienced practitioners. This impact should be mitigated by providing clear expectations for members of the public in advance (e.g. if waiting times/consultation times are likely to be extended). Programs should ensure safety and welfare are not compromised while waiting.
VCE staff working in training programs should have supervisory roles and instructional training and skills. Providing services to pets from populations that are underserved does not warrant less supervision than other settings. VCE programs often require more safety mechanisms and oversight than standard or specialty care facilities due to the ethical considerations of choice and access to care. The onus falls on instructors to provide trainees with the tools to effectively engage families in healthcare decision-making and provision of care while incorporating animal welfare principles and consideration for quality of life.11 Achieving this balance is made easier by establishing clear protocols and decision-making tools for providing care within the scope and capacity of the program. Additionally, programs must ensure consistent training and support, supported by protocols for teaching in addition to clinic operations, procedures, inventory, and communications which are shared with trainees.
Trainees delivering medical care should be under the direct supervision of an experienced and licensed veterinary professional and have demonstrated competence in relevant skills for the clinic or activity prior to participating in a clinical setting. These skills include aspects of clinical care, client counseling, and decision-making. Many students get their primary hands-on experience through animal and human populations at shelters or in community work. If a student is not allowed to perform procedures without direct supervision in other settings, those restrictions should not change simply because a client has fewer resources. Students are not a substitute for a trained professional.
Trainees’ technical competence should be assessed on models or simulations prior to performing procedures on live animals. Supervisors should ensure students have the appropriate skills, such as giving injections, knot-tying and sterile technique, in advance, and should ascertain students’ level of experience prior to case assignment. When surgical procedures are part of a program’s healthcare delivery, it is essential to safeguard animal welfare by ensuring anesthetic and surgical times (and consequent risks of complications) are not excessive. It may be more appropriate to allow a less experienced student to scrub in or lead on a single part of the procedure initially, rather than prolonging the surgical time for them to complete a full procedure. Procedural time limits can help ensure patient safety and welfare, and support student learning. Likewise, surgical intervention without appropriate sterility and pain relief or performing exploratory surgery for teaching purposes is not acceptable.
Trainees can benefit from seeing how successful partnerships are formed and fostered over time by participation in this work. Likewise, trainees are more likely to benefit from repeated opportunities for modeling clinical and communication skills development. Program supervisors should include longitudinal tracking to ensure risk mitigation and quality of care are not compromised.
Finally, special attention should be paid to any hidden culture or curriculum21 that may influence interested parties’ interactions and that could be damaging to partner communities. Training programs engaging with historically underserved populations require a more robust examination of systems in place to ensure damage is not being done to the community or animals. For example, spay-neuter student training programs should not result in animals staying longer in the shelter or other institutional settings than they would otherwise.
Establishing requirements for trainees to participate in VCE training programs
A full-spectrum training approach facilitates productive relationships and comprehensive learning and program outcomes. A publication by Rivkin-Fish22 describes a dentistry training program in a lower income community and ethical concerns surrounding trainee attitudes and engagement in what is a ‘commodified healthcare system’. Students reported perceptions such as ‘deserving to get experience’ and not wanting to do ‘boring’ things and sometimes questioned the level of investment of patients based on their health status. Rivkin-Fish22 emphasized the importance of building in elements to provide for more comprehensive training experiences in community work: providing faculty supervision, meeting client needs while recognizing the limitations of services offered, discussing the full spectrum of treatment options, and recognizing that social justice, and not altruism, is the basis for this work.
This discussion translates well to the veterinary field. Orientation/training programs identify the goals of the community work and mitigate ‘savior’ mentality/complex, which can be found in both novice and experienced participants. Training can ensure that community-based teaching programs directly discuss the causes of health disparities and more actively address troubling attitudes and misconceptions. A thoughtful integration of training items can be useful (see Fig. 3.3).
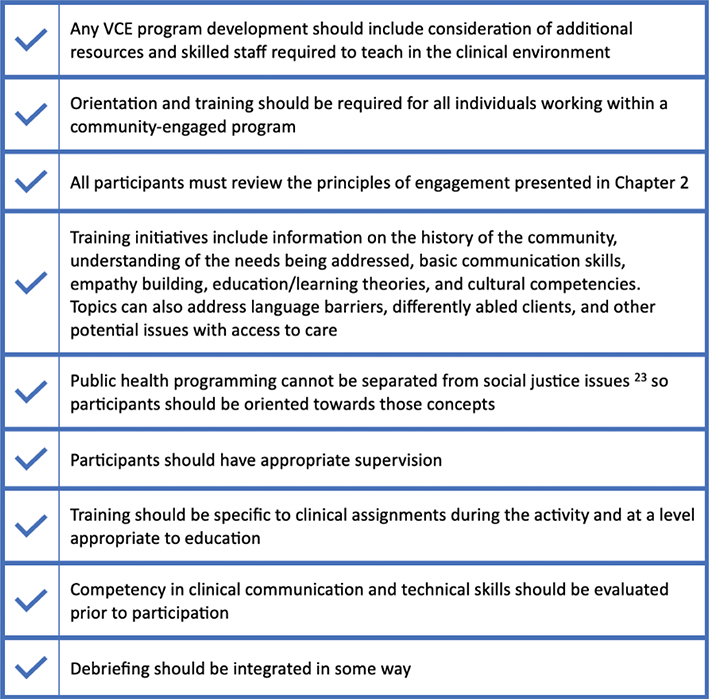
Fig. 3.3. Checklist of elements to consider in veterinary community engagement (VCE) training programs. These items are not intended to be completed in any particular order but should be incorporated in VCE settings that provide training.
Training in best practice VCE should not only be required of students in academic programs, but of any program employee or volunteer. Starting with an emphasis on the goals of the program, training can illustrate ethical issues associated with one-time events or those focused on publicity, rather than those providing a sustainable partnership with the community itself. It can also help ensure that the needs of the community are not negatively impacted by the participation of volunteers or students.
Specific implications for core curricular VCE training programs in academic partnerships
When including community initiatives as part of the core or required curriculum, it is essential to anticipate the points at which the curricular requirements could potentially conflict with the needs of the community and create a contingency plan. Given this engagement experience is core material, all students, regardless of their skill level, experience, or interest, would be required to engage. These experiences can inappropriately prioritize student experience and productivity over other participant needs and can contribute to students’ (incorrect) perceptions that their experience is more important than other participants’ or that they have a ‘right’ to perform procedures on animals in these populations.
Specific implications for extracurricular student training and activities
Trainees may gain valuable experiences from extracurricular and volunteer activities related to veterinary medicine. In fact, many veterinary colleges rely on student clubs and other extracurricular activities to provide clinical experiences beyond what can be provided by the core curriculum. It is essential these experiences are subject to the same ethical review, requirements, supervision, and expectations for animal welfare as core institutional experiences.
Academic institutions and other organizations have a responsibility to ensure that proper oversight exists even for activities not directly funded or directed by the organization, such as student clubs or volunteer tourism events. As with core educational programs, extracurricular clinical experiences require oversight by licensed professionals and should not permit students to participate in clinical activities without demonstrating competence in basic skills. The participation of trainees should only be at the level permitted by their level of education as outlined in relevant regulations.
Special considerations for international work
Cultural humility is critically important for all programs, including international work. Navigating different geographic or cultural restrictions, legal requirements, supervision of trainees, and ensuring volunteer training are all requirements for international VCE programs. Some settings for international engagement may not require a high level of oversight in their veterinary regulations; nonetheless, the ethical considerations are the same.
Student work should be particularly scrutinized, observed, and mentored by those who are competent in their field. For example, students involved in surgical programs should be directly mentored by a representative veterinary trainer who is competent not only in surgery but in training and ethical implications of community work in that location. Whenever possible, local professionals should be employed by programs to bridge cultural and technical gaps and provide for increased sustainability.
Mistakes will be made: address them ethically and in a reflective manner
VCE programs are charting new territory and will make mistakes. Programs should provide honest acknowledgement and reflective evaluation of those mistakes. Changing course and/or debriefing on what occurred is part of responsible community engagement. Reporting systems to capture errors and responses should exist within a supportive environment.24
Veterinary professionals are subject to fears of liability. As a profession, veterinary medicine is increasingly risk averse; some of this is driven by specialty and academic practice, as well as social media pressures.25 The increasing gap in AVC and the need for more accessible community medicine programs require that programs take measured risks in order to improve community animal health and welfare. Proactive, thoughtful program design, clear communication, and support from within the profession can counteract risks and fears of liability.26
References
| 1. | The Association of Shelter Veterinarians. Position Statement: Veterinary Supervision in Animal Shelters. https://www.sheltervet.org/resources/position-stmts. Accessed April 14, 2023. |
| 2. | Carpenter-Song EA, Schwallie MN, Longhofer J. Cultural competence reexamined: critique and directions for the future. Psychiatr Serv. 2007;58(10):1362–1365. doi: 10.1176/ps.2007.58.10.1362 |
| 3. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 4. | Brandt AM. Racism and research: The case of the Tuskegee Syphilis Study. Hastings Cent Rep. 1978;8(6):21–29. https://doi.org/10.2307/3561468 |
| 5. | Washington HA. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans from Colonial Times to the Present. Doubleday Books; 2006. |
| 6. | Park M, Lee M, Jeong H, Jeong M, Go Y. Patient-and family-centered care interventions for improving the quality of health care: a review of systematic reviews. Int J Nurs Stud. 2018;87:69–83. doi: 10.1016/j.ijnurstu.2018.07.006 |
| 7. | Brown CR, Edwards S, Kenney E, et al. Family quality of life: pet owners and veterinarians working together to reach the best outcomes. J Am Vet Med Assoc. 2023;1(aop):1–6. doi: 10.2460/javma.23.01.0016 |
| 8. | NEJM Catalyst. What is patient-centered care? NEJM Catalyst. 2017;3(1). doi: 10.1056/CAT.17.0559 |
| 9. | Mellor DJ, Beausoleil NJ, Littlewood KE, et al. The 2020 five domains model: including human–animal interactions in assessments of animal welfare. Animals. 2020;10(10):1870. doi: 10.3390/ani10101870 |
| 10. | Riemer S, Heritier C, Windschnurer I, Pratsch L, Arhant C, Affenzeller N. A review on mitigating fear and aggression in dogs and cats in a veterinary setting. Animals. 2021;11(1):158. doi: 10.3390/ani11010158 |
| 11. | Grimm H, Bergadano A, Musk GC, Otto K, Taylor PM, Duncan JC. Drawing the line in clinical treatment of companion animals: recommendations from an ethics working party. Vet Record. 2018;182(23):664. doi: 10.1136/vr.104559 |
| 12. | Ringler T, Ahearn EP, Wise M, Lee ER, Krahn D. Using life stories to connect veterans and providers. Fed Pract. 2015;32(6):8–14. |
| 13. | Shaver SL, Larrosa M, Hofmeister EH. Factors affecting the duration of anesthesia and surgery of canine and feline gonadectomies performed by veterinary students in a year-long preclinical surgery laboratory. Vet Surg. 2019;48(3):352–359. doi: 10.1111/vsu.13163 |
| 14. | Straubhaar R. The stark reality of the ‘white saviour’ complex and the need for critical consciousness: a document analysis of the early journals of a Freirean educator. Compare J Compar Int Educ. 2015;45(3):381–400. doi: 10.1080/03057925.2013.876306 |
| 15. | Bowman N, Brandenberger J, Lapsley D, Hill P, Quaranto J. Serving in college, flourishing in adulthood: does community engagement during the college years predict adult well-being? Appl Psychol Health Well Being. 2010;2(1):14–34. |
| 16. | Horecka K, Neal S. Critical problems for research in animal sheltering, a conceptual analysis. Front Vet Sci. 2022;9:804154. doi: 10.3389/fvets.2022.804154 |
| 17. | Neumann SL. Animal welfare volunteers: who are they and why do they do what they do? Anthrozoös. 2010;23(4):351–364. doi: 10.2752/175303710X12750451259372 |
| 18. | Hustinx L, Grubb A, Rameder P, Shachar IY. Inequality in volunteering: building a new research. Front Voluntas. 2022;33(1):1–17. doi: 10.1007/s11266-022-00455-w |
| 19. | Jackson A, Kania J, Montgomery T. Effective change requires proximate leaders. Stanf Soc Innov Rev. 2020. |
| 20. | American Association of Veterinary Medical Colleges (AAVMC). VMCAS 2023 Applicant Guide. https://www.aavmc.org/wp-content/uploads/2022/01/AAVMC-VMCAS2023-Applicant-Guide.pdf. Accessed April 17, 2023. |
| 21. | Roder CA, May SA. The hidden curriculum of veterinary education: mediators and moderators of its effects. J Vet Med Educ. 2017;44(3):542–551. doi: 10.3138/jvme.0416-082 |
| 22. | Rivkin-Fish M. Learning the moral economy of commodified health care: ‘community education’, failed consumers, and the shaping of ethical clinician-citizens. Cult Med Psychiatry. 2011;35:183–208. doi: 10.1007/s11013-011-9208-0 |
| 23. | Gostin LO, Powers M. What does social justice require for the public’s health? Public health ethics and policy imperatives. Health Affairs. 2006;25(4):1053–1060. doi: 10.1377/hlthaff.25.4.1053 |
| 24. | The Veterinary Defence Society. VetSafe. https://www.vds-vetsafe.co.uk. Acceaaed April 7, 2023. |
| 25. | Paul M. Divided We Fall: Nonprofit Facilities and for-Profit Veterinary Clinics Seem Constantly at Odds. https://www.dvm360.com/view/divided-we-fall-nonprofit-facilities-and-profit-veterinary-clinics-seem-constantly-odds. Accessed April 14, 2023. |
| 26. | Brown CR, Garrett LD, Gilles WK, et al. Spectrum of care: more than treatment options. J Am Vet Med Assoc. 2021;259(7):712–717. doi: 10.2460/javma.259.7.712 |
Chapter 4: Managing organizational support for veterinary community engagement
Key objective: This chapter illustrates elements of structural capacity present in community-engaged programming and their specific applications to VCE programming; these elements include financial, personnel, and capacity factors. The list of considerations is long, so brief summaries and main points are included in the chapter, with further resources and reading indicated where appropriate.
Introduction
Principles of Community Engagement provides frameworks to guide organizations in understanding ‘...the capacity they need to support community engagement’1 which includes the structural capacity categories from Handler, Issel and Turnock.2 Further described in Birkhead, Morrow and3 Turnock’s Public Health: What It Is and How It Works (7th edition), the capacity resources, or inputs, needed by health systems for public health functions are: human resources, fiscal and physical resources, information resources, and organizational resources, and these can be applied across organizations.3 (see Table 4.1).
| Resource Category | Descriptive Examples |
| Fiscal | Management of finances, type and amount of funding available, funding timelines, and requirements |
| Human | Individuals and the skills, knowledge, and training they bring to the activity |
| Physical | Physical space, supplies, and equipment |
| Information | Data on community demographics, existing services, and efficacy of proposed interventions |
| Organizational | Management of partnerships and administrative needs, logistics, and reporting |
Developing effective programs must include identifying, analyzing, and committing to required resources: time, personnel, expertise, and financial support. Two of the most necessary resources for organizational support in VCE programming are fiscal power and people power. It is not enough to have the funds to implement a program, nor is it enough to have a surplus of passion, energy, and community relationships without the means to provide supplies and structure to channel these into an ongoing and sustainable program. Both components are obviously essential for starting and sustaining programs.
Financial considerations
The veterinary industry was developed as a fee for service model with rare exceptions; it is increasingly recognized that traditional for-profit practice models largely serve the affluent.4 The idea of a non-profit organization as a provider of veterinary care has been controversial in the United States in many places; this resistance is exemplified by a number of state veterinary practice acts that specifically prohibit animal shelters and other non-profit organizations from providing veterinary care to owned animals, either entirely or with strict guidelines regarding scope and conditions under which it can be provided.5,6
Over time, animal shelters and non-profit animal welfare organizations have played an increasing role in the provision of affordable veterinary care, first focusing on preventive medicine services (e.g. spay-neuter and vaccinations) but more recently expanding into more comprehensive services.7,8 Despite hundreds of US veterinarians now working in shelters, spay/neuter clinics, and low-cost clinics, accessible care remains controversial. Many VCE programs delivering veterinary care have been established to fill care gaps as part of growing access to care movement; others have been built to address the need for training opportunities for veterinary and technical students.
For-profit clinics with a low-cost or affordable pricing structure are also increasingly common, resulting in an emerging field often referred to as Access to Veterinary Care (AVC) that straddles traditional boundaries between non-profit and for-profit practice. Different financial structures within the non-profit sector include independent clinics, a non-profit branch of a for-profit clinic, or use of a larger non-profit as a fiscal sponsor of the clinic (this can be a particularly helpful way for a new organization to get started).4
Programs must have a well-reasoned business model and a plan for sustainable funding. These can vary greatly between programs, and usually involve several components (Table 4.2).
Grant funding which includes requirements or growth that does not align with other resource categories or programmatic goals can inadvertently have a negative impact on communities. VCE programs are more effectively planned with several years of sustained funding rather than in reaction to short-term funding opportunities. Funding organizations are specifically encouraged to commit support over periods more conducive to authentic partnerships, such as years, and to look for VCE projects in line with these principles.
Failing to plan for sustained funding can also compromise overall organizational health as well as limit opportunities for growth. These plans should enroll the community as contributors to the extent that is reasonable and realistic. For example, even in underserved communities, the concept of fee-for-service (asking pet owners to make a financial contribution toward their pet’s cost of care) can be considered. While every organization and program must decide what the best approach is, financial contributions from pet owners can be an important pillar of financial stability.
VCE programs are encouraged to explore varied approaches to fee-for-service models, borrowed from existing clinics and other industries. Such approaches can include subsidized costs with flat fees for services, pay-what-you-can models where pet owners are given the flexibility to pay some, all, or more than the cost of services, and the use of payment plans (among others). While payment plans can carry a large amount of administrative cost, recent studies suggest that this can be mitigated with the use of third-party programs and furthermore show a great opportunity for extending the financial reach of limited donations or funding.9 Care should be taken with third-party payment options to ensure they are acting in the best interest of the community member and not predatory lending programs, historically targeted at BIPOC and lower income borrowers.10
Person power
People are the most valuable, and often costly, resource. As described in Chapters 1 and 2, the identification of community assets, including human resources, is an essential component of VCE. Proximate leaders and community members should be recruited early and actively enrolled in planning. Programs should aim to hire and provide a living wage for community members whenever possible. While employing community members is one of the most important elements of sustainability, salaries tend to be one of the most difficult elements to fund, especially in regard to grants or donor dollars. Balancing this duality is one of the great challenges of programming.
The breadth of human resources needed to support VCE programming depends on several factors, including the scope of medical services provided, frequency of offerings, support needed for funding and financial planning, among others. Roles range from administrative staff for executing logistical needs to veterinary professionals (e.g. technicians, assistants, and veterinarians) for delivering medical services. Planning for role support and staffing should occur early in the development of a program, as well as in response to early successes and challenges.
Programming must comply with veterinary practice standards, licensure, and local regulations. While VCE projects do not require compensation for medical team members, it does require that only those with the appropriate credentials, training, and expertise are given these responsibilities (see Table 4.3 for additional key roles people may play in VCE programs).
Financial considerations of reliance on volunteers in VCE programming
The ethical considerations of relying on volunteers to execute programming were discussed in Chapter 3. These concerns dovetail with potential financial liabilities. Appropriately incorporating a volunteer workforce requires a substantial investment of resources, including training, supervision, and management.
The roles served by proximate leaders generally warrant compensation or other support, which can better support overall program goals and outcomes. Enrolling members of the community in compensated, supported roles with adequate time and concentration on the work not only builds stronger foundational relationships but also invests back in the community and makes for more authentic partnerships. Overdependence on volunteer labor may compromise the sustainability of the program in the community.
VCE programs delivering veterinary services require specific skill sets from professionals who may already be tapped in many other places. Professional volunteers may be battling with burnout, stress, and professional fatigue.11 Relying on professional volunteers to carry out this work is likely to become problematic over time, especially if these volunteers are also given administrative tasks better provided by community members and/or salaried employees.
Additional considerations: informational, physical, and organizational resources
Human and fiscal resources are often addressed in the planning stages of VCE programming. Additional structural resources need to be addressed for the implementation of VCE initiatives. The other core components of public health infrastructure are informational, physical, and organizational resources.1,2
Informational resources encompass a wide range of categories which at their core are data or knowledge-based. Examples of information resources include procedural information, such as clinical protocols, logistics of care delivery, and efficiency models in programming. Other examples include community information, including identified needs and assets, methods for managing those needs and assets, identification of participants, and community programs and dynamics that may impact the success or failure of the program. Often accessing information resources involves partnership and trust in addition to just exchanging information.
Physical resources include the supplies needed for the provision of services. For VCE programs, this means materials and equipment for veterinary medical and surgical care, technical resources such as equipment and systems for recordkeeping, goods provided to pet owners and community members, and other tangible supplies. They also include facilities for providing care, whether in brick-and-mortar locations, mobile units, vehicles, or temporary spaces for MASH clinics.
Organizational resources involve collaborations and partnerships for executing programs and logistical, management, and administrative needs. Examples may include access to grant writers to allow for more direct efforts in applications, partnerships with community organizations that share administrative tasks, or structuring a Board of Directors for oversight. Decisions about organizational structure may determine the function of leadership; a fundraising board focused on financial support plays one role in organizational stability, while an executive board provides programmatic direction with a different impact on the organization.
Resource categories need to be considered holistically. For example, cultural humility training for staff, volunteers, and partners would fall under informational resources but it needs to be accounted for in administrative time and financial budgeting. Facility use may fall under an in-kind donation if provided by a partner, but maintenance staffing or renovation efforts land in other resource categories.
Sustainability
Often, the goals of a VCE program are to have a lasting impact and program repeatability. Ideally, VCE programs, whenever possible, utilize resources and materials readily available in the community. As discussed, the utilization of local professionals, volunteers, and trainees is more likely to sustain an effort over time. Programs that require transporting large numbers of people and materials should collaborate with community members to determine how to minimize waste and environmental impact and integrate training and development of community members, as essential aspects of program development.
Sustainability also means being realistic about the program’s capacity for care. This concept is utilized in the animal shelter medicine field and describes the shelter’s ability to meet the needs of animals using available resources. Resources that constrain a shelter’s capacity for care include finances, time, personnel skills, housing and other physical resources, and opportunities for providing live outcomes in the shelter system.12 In the same way, capacity for care applies in animal sheltering, VCE work must guarantee programs, have the resources necessary to provide the animal health services offered or adjust program scope and expectations. Failure to work within the capacity for care overextends the organization, jeopardizes trust, compromises patient care, allows for mission creep, and negatively impacts the health of personnel and communities.
References
| 1. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 2. | Handler A, Issel M, Turnock B. A conceptual framework to measure performance of the public health system. Am J Public Health. 2001;91(8):1235–1239. doi: 10.2105/ajph.91.8.1235 |
| 3. | Birkhead GS, Morrow CB, Pirani S. Turnock’s Public Health: What It Is and How It Works. 7th ed. Jones & Bartlett Learning; 2020. |
| 4. | Haston RB, Pailler S. Simulation of the effect of low-cost companion animal clinics on the market for veterinary services. Am J Vet Res. 2021;82(12):996–1002. doi: 10.2460/ajvr.21.08.0116 |
| 5. | Fiala J. Veterinary Nonprofits: Unfair Competitors or Worthy Charities? VIN News Services. https://news.vin.com/default.aspx?pid=210&Id=6256827&useobjecttypeid=10&fromVINNEWSASPX=1. Accessed August 24, 2023. |
| 6. | Paul M. Divided We Fall: Nonprofit Facilities and for-Profit Veterinary Clinics Seem Constantly at Odds. https://www.dvm360.com/view/divided-we-fall-nonprofit-facilities-and-profit-veterinary-clinics-seem-constantly-odds. Accessed April 14, 2023. |
| 7. | Bushby PA. High-quality, high-volume spay–neuter: access to care and the challenge to private practitioners. J Feline Med Surg. 2020;22(3):208–215. doi: 10.1177/1098612X20903600 |
| 8. | Garabed R, Overcast M, Behmer V, Bryant E, Heredia K, Jones A. Business models used to improve access to veterinary care. 2022. https://www.aspcapro.org/sites/default/files/2022-05/business-models-used-to-improve-access-to-veterinary-care.pdf. Accessed August 24, 2023. |
| 9. | Cammisa HJ, Hill S. Payment options: an analysis of 6 years of payment plan data and potential implications for for-profit clinics, non-profit veterinary providers, and funders to access to care initiatives. Front Vet Sci. 2022;9:1091. doi: 10.3389/fvets.2022.895532 |
| 10. | Goldstein D. Understanding Predatory Lending: Moving toward a Common Definition and Workable Solutions. Neighborhood Reinvestment Corporation; 1999. |
| 11. | Merck Animal Health. Merck Animal Health Veterinary Wellbeing Study III. https://www.merck-animal-health-usa.com/about-us/veterinary-wellbeing-study. Accessed August 24, 2023. |
| 12. | The Association of Shelter Veterinarians (ASV). The guidelines for standards of care in animal shelters: second edition. J Shelter Med Commun Animal Health. 2022;1:1–76. doi: 10.56771/ASVguidelines.2022 |
Chapter 5: The value of social networking in veterinary community engagement
Key objective: This chapter explores the concept of social networking, which recognizes and utilizes existing connections and relationships in communities in order to optimize the delivery of community-engaged programming.
Introduction
To authentically engage communities, it is essential to recognize the existing connections and relationships that exist within the fabric of every community. Communities are not made up of an unrelated set of individuals, but rather by groups of individuals with connections between them. This usage of the term social networking in this chapter is different from the phenomenon of ‘social networking’ as it applies to the digital space, which is also a critical tool for community engagement.
Defining social network
A social network consists of a finite set of actors and the relation or relations between them.1 Any individual in a community can be part of numerous such networks. A network is more than traditional relationships such as family, tribe, or clan; networks also consist of connections formed through proximity (e.g. landlord, housing associations), religion (e.g. churches and faith-based groups), educational programming (e.g. schools), or recreational activities (e.g. sports, hobbies).
In the field of human healthcare, it is well known that an individual’s social networks play an important role in their health.2 Social networks can influence an individual’s health negatively such as increasing their risk for obesity, smoking, or drug use, or may have a positive impact such as buffering them from stress or motivating individuals to increase physical activity. While not all experts agree on how social networks impact human health, whether or not social networks impact animal health and welfare has not been explored.
Engaging social networks
In human healthcare, leveraging social networks is a known strategy used in interventions designed for health improvement. The concept of social capital includes features of social organization such as networks, norms, and social trust that facilitate coordination and cooperation for mutual benefit.3 Social capital can be used to facilitate health improvement efforts.
Some work in the field of human interactions has suggested that pets themselves can serve as social capital.4 Human service agencies therefore may seek to engage community members through their pets5 which presents an opportunity for collaboration between animal service organizations and human social services. Social networks can be engaged to provide feedback and to identify priorities or opportunities to establish a plan for intervention.
Building and sustaining networks of individuals and entities for community engagement involves establishing a communications channel, exchanging resources, and coordinating collaborative activities.6 Strengthening existing relationships and building new ones mobilize community members to take action.
Recognizing community resources
Outside of animal welfare and veterinary medicine, existing human service providers and professionals are already engaged in providing support to community members, many of whom are also pet owners. There are many ways of engaging with communities that have nothing to do with pets or healthcare; however, leveraging existing frameworks can be an important way of reaching pet owners. Moreover, the human-animal bond can be a powerful motivating force which can increase community member engagement.7
Tapping into a community’s networks
As discussed in Principle 1, becoming knowledgeable about the community means actively exploring the community’s cultures and institutions, its capabilities and assets, and its health needs and challenges. Typically, learning about a community requires a variety of approaches, including gathering existing data and generating new information, combining qualitative and quantitative data, and incorporating the perspectives of a broad spectrum of individuals, organizations, and groups. Understanding a community’s social networks is essential because of their potential to affect population health (Table 5.1).
| Conduct a needs and strengths assessment prior to planning a new program |
| Identify appropriate community partnerships including existing veterinary resources in the area and what barriers they are able to overcome and which they have not yet |
| Reach out directly to other agencies and meet with leadership |
| Attend community meetings to better understand community viewpoints and increase relationship-building |
| Attend neighborhood events |
| Adapted from CDC.6 |
Examples of other service providers working in communities include social workers, housing assistance agencies, neighborhood watch, climate activists, walk/bike community activists, social justice movements, school systems, food assistance programs, fuel assistance, church groups, community meetings, government, and non-government organizations. These can also be part of the community’s social network.
Digital social networking
While not the focus of this chapter, the document would not be complete without acknowledging the ‘other’ type of social networking: social media and digital platforms such as Facebook, Instagram, and X (formally known as Twitter). There are certainly pros and cons to using social media as a tool in community engagement8; veterinary community engagement (VCE) programs need to be aware of the potential for harm but may successfully engage such platforms to advance their work. The use of social media in veterinary medicine has recently been reviewed.9
Aside from being an important communication tool, social media can be an active community space. Many fundraising efforts are now based on social media platforms and can attract a lot of interest. Social media is also useful for reaching youth and those connected to educational platforms. Social media used for good can also have a democratizing effect of allowing everyone to provide an opinion.
VCE programs utilizing social media are advised to include precautions for privacy and to frequently monitor comments on platforms to mitigate the potential for harm. In particular, digital media can raise questions of trust and security. Social media platforms should be used to enhance other community engagement efforts, not replace them.
Social networks are integral pieces of the community fabric and may be informal as well as formal. All are important and should be examined and considered during each stage of program development, implementation, and review. A successful organization that can respond to community needs is able to navigate these relationships with flexibility and self-awareness, allowing for changes and responses as new challenges develop, new information is learned, and the community landscape shifts over time.
References
| 1. | Wasserman S, Faust K. Social Network Analysis: Methods and Applications. Cambridge University Press; 1994. |
| 2. | World Health Organization (WHO). Social Determinants of Health. https://www.who.int/health-topics/social-determinants-of-health. Accessed April 7, 2023. |
| 3. | Putnam R. Bowling alone: America’s declining social capital. J democr. 1995:6(1):65–78. |
| 4. | Wood L, Giles-Corti B, Bulsara M. The pet connection: pets as a conduit for social capital? Soc Sci Med. 2005;61(6):1159–1173. doi: 10.1016/j.socscimed.2005.01.017 |
| 5. | Jennings BM, Lem M, Kilborn S, Donnelly B, Acker A. Improving oral health care accessibility for homeless and vulnerably housed pet-owning populations. Can J Dent Hyg. 2022;56(2):98. |
| 6. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 7. | Human Animal Support Services. Community Partnerships. https://www.humananimalsupportservices.org/toolkit/community-partnerships/. Accessed August 14, 2023. |
| 8. | Ventola CL. Social media and health care professionals: benefits, risks, and best practices. Pharm Therapeut. 2014;39(7):491–499, 520. |
| 9. | DeWilde C. Social media and digital marketing for veterinary practices. Vet Clin. 2024;54(2):381–394. doi: 10.1016/j.cvsm.2023.10.006 |
Chapter 6: Programmatic evaluation of veterinary community engagement and challenges in community-based research
Key objective: This chapter applies and refines the process of program evaluation (planning, implementation, completion, dissemination, and reporting) as outlined in the Principles of Community Engagement 2nd edition1 to the practice of veterinary community engagement (VCE).
Introduction
Many interested parties in community-engaged work will want to collect information about the program’s impact. This information might be used for program evaluation, to support funding applications, to meet grant requirements, or to contribute to a general body of knowledge beyond that individual program. Participants may have different goals. For example, academic programs place a high value on the publication of findings, and publication can be an important aspect of career development and growing expertise in the field. Animal welfare organizations may be highly motivated to support the goals of their funders. Community members may be interested in the quality of service delivery. Fortunately, formal program evaluation, including that which is also accomplishing scholarly research, can meet all these goals when conducted ethically.
Program evaluation
Program evaluation is a key element of any public health intervention.2 Providing this type of evaluation of efficacy and objectives is an essential responsibility of any program. The concept of pragmatically evaluating how a program or protocol works and then adjusting based on that information is important not just in clinical community work, but also in other areas including education and emergency preparedness. The emergency preparedness cycle (see Fig. 6.1) at its core is about planning, organizing, training, performing the action (whether through an actual response or training exercise), and then evaluating and improving the process. This cycle model is representative of a foundational concept in public health that programming allows for open communication and productive change over time.
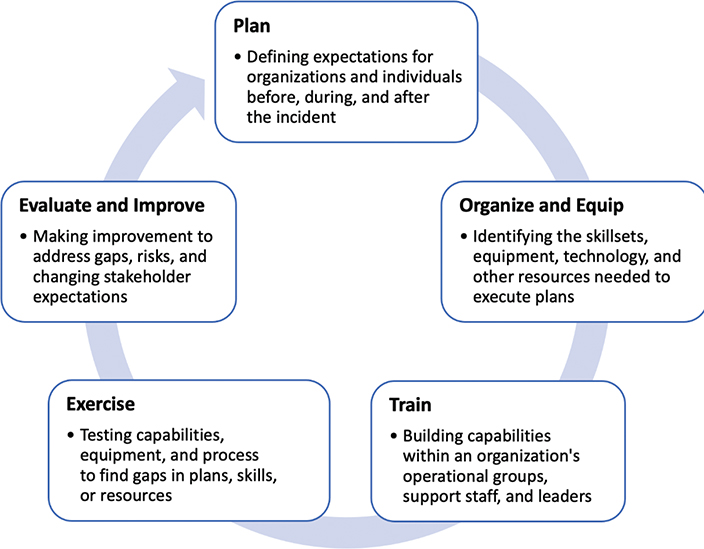
Fig. 6.1. The emergency preparedness cycle which involves planning, organizing, training, performing the action, and evaluating and improving the process. Diagram adapted from FEMA (Federal Emergency Management Agency3).
Evaluation is also important to educational efforts in the classroom and is often discussed under the concept of ‘action research’. This model (see Fig. 6.2) shows a similar process including planning a particular intervention, doing the intervention, observing and gathering information about how it is going, reflecting on that information, and then finally integrating new information into a revised plan. Action research, such as program evaluation, is not necessarily generalizable, although it can be, and is intended to be used for immediate application.4
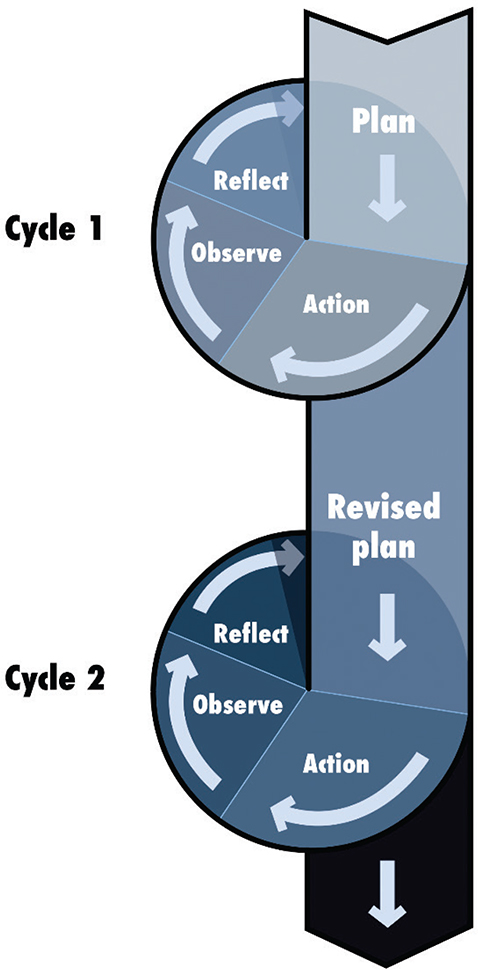
Fig. 6.2. Action research model, adapted from Burns,5 which involves planning an intervention, doing the intervention, observing, and gathering information about how it is going, reflecting on that information, and then integrating new information into a revised plan.
Core considerations in this work include protecting vulnerable populations, including students, minors, or other groups. Doing ‘no harm’ and avoiding inaccurate representations6 is critical, as well as not putting participants at risk and providing accurate disclosures.7 This framework can also be used to understand public health interventions through concepts such as community-engaged pedagogy, which includes building partnerships, developing learning communities, adjusting, and researching.8
In VCE programs, this cycle of critical thinking, evaluation, and adjustment is essential to protecting partnerships and measuring impact. It also helps establish reasonable expectations, open communication about adjustments, and the anticipation of adjustments over time for all parties involved, based on new knowledge and changing needs. Integrated into initial planning are identifying and understanding interested parties, their expectations for program impact, and methods for evaluating success (Principle 9).
Different interested parties are likely to have different goals (Principle 6). Open recognition of the potential for competing priorities enables productive communication and ethical programming. Open discussion and engagement in this evaluation process also ensures that all participants are aware of changes or adjustments as they are made and that accurate conclusions are being drawn from program efforts. Findings also inform future interventions and programming.
Types of evaluation
Evaluation should involve stakeholders in the process through approaches such as participatory or empowerment-based evaluation.1 Basic evaluation types include qualitative, quantitative, or mixed methods and all or a combination might be used in all different stages of a project (see Fig. 6.3). Mixed methods are common in this type of work to try to gain a more holistic view of program impact, but any evaluation methods should align the questions being asked and project impact.
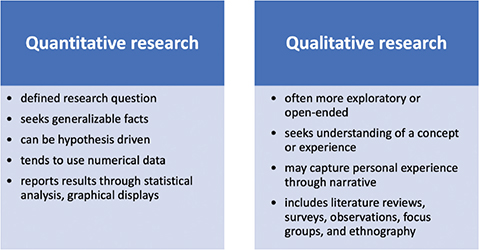
Fig. 6.3. Quantitative and qualitative questions that may guide program evaluation during program planning, implementation, and when assessing program outcomes. Adapted from CDC1 (Table 6.1).
Because this information will be used to inform programming, particularly in historically underserved populations, it is important that study methods are appropriate and that conclusions are as accurate as possible. Overstating impact does not serve any of the interested parties. Program evaluation and traditional academic research share methodology; there can be significant overlap in the processes of program evaluation and research design and reporting.
| 1. Engaging and maintaining community involvement |
| 2. Overcoming differences between and among academics and the community |
| 3. Working with communities not traditionally served by the veterinary or animal welfare professions |
| 4. Initiating a project with a community and developing a community advisory Board |
| 5. Overcoming competing priorities and institutional differences |
| Adapted from CDC.1 |
The role of research in VCE programs
Program evaluation provides donors and other interested parties with information about program impact and outcomes and allows for programmatic evolution and improvements. Additionally, academia and other fields of inquiry also value knowledge for its own sake. University faculty are often required to conduct scholarly research in part because of the high value placed on contributions to a larger body of knowledge. Many theories of change also grow from foundational knowledge that supports the need for action.9
Scientific inquiry is grounded in the philosophy of positivism, which is the idea that there is a knowable reality that exists independent of the research process. VCE programs have the goal to translate knowledge into improved animal and community health and to meet objectives determined by all interested parties. By having a better understanding of a problem and its root causes as well as the impact of solutions, programs are better equipped to address the problem. In addition, data collection can also help ensure resources are used wisely.
For veterinary medicine specifically, research is vital to helping develop the new field of accessible veterinary care (AVC). For example, developing the evidence base for effective low-cost treatment options is essential to helping to lower the cost of care and support the spectrum of care and contextualized care approaches. The principles of evidence-based medicine10 suggest that treatment options can be defensible and can protect programs and practitioners from unsubstantiated concerns about ill-defined veterinary practice standards.
Research funding is often available from the government or other funding agencies, particularly for social or healthcare challenges impacting people. Thus, VCE programs might choose to participate in research projects as a means to obtain funding for general program support. Finally, citizen science is another way to engage members of a community around a policy issue or community need. In the citizen science model, data are directly collected by members of the public.11 Just as training programs need to conduct regular programmatic evaluations (see Chapter 3), regular evaluation of research goals and programmatic impact helps determine what needs to be added, discontinued, or improved.
Data collection for research
Methods for collecting data for research mirror those previously described for program evaluation. Indeed, program evaluations can be the central focus of a VCE research project. For example, academic training programs may use program evaluations as material for publishing student perceptions and learning outcomes from a VCE project. However, VCE research often seeks to answer questions beyond programmatic variables. Research methods, such as program evaluation, can include quantitative, qualitative, or mixed-methods research methodologies. Methodology, in turn, impacts how data are analyzed and ultimately published (see Fig. 6.4). As in evaluation, research can also employ mixed methods in study design.
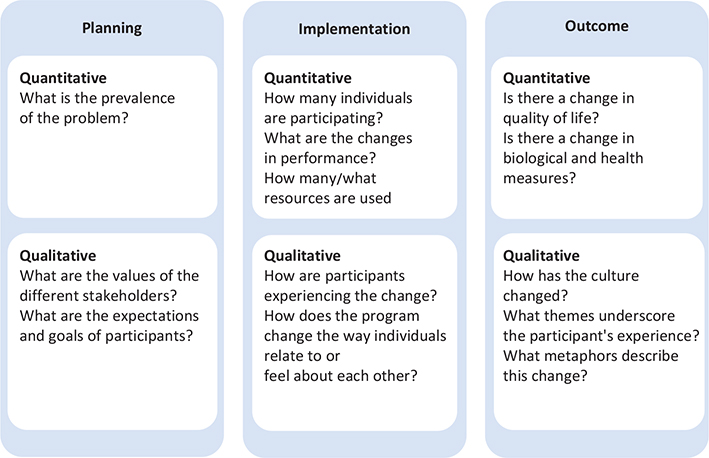
Fig. 6.4. Fundamental elements of quantitative and qualitative research methodologies. Adapted from the Association for Qualitative Research (AQR).12
Challenges in community-engaged research
Conducting research in collaboration with a community partner can present several challenges. Ideally, research will be community-led, meaning that the research questions are developed by community leaders and interested parties who are motivated to learn the results. Researchers must avoid imposing their own agenda upon a community or project.
Community-based participatory research as a solution to challenges
In human medicine, community-based participatory research (CBPR), as defined by the National Institutes of Health (NIH), is community-based research in public health focused on social, structural, and physical environmental inequities through active involvement of community members, organizational representatives, and researchers in all aspects of the research process. Partners contribute their expertise to enhance understanding of a given phenomenon and to integrate the knowledge gained with action to benefit the community involved.13
A key aspect of authentic CBPR is that the research question was developed by the community. In reality, most projects involve a lot of direction by research partners based in academia or human service agencies. While a separate discipline of veterinary CBPR does not yet exist, many programs seek to apply CBPR principles to their work and strive to include community leaders as members of the research team.
Research ethics
Research ethics are particularly important to consider when conducting formal research in community work as well as program evaluation. Although legal requirements may not extend to individual program evaluation, consideration of the ethics and disclosure process should be considered for both formal research projects and program evaluation. Community members may be distrustful of research given historical links between scientific research and the oppression of underrepresented groups; the onus is on the researcher to recognize historical failures and oversights and endeavor to correct past mistakes (Principle 3).
Scientific contributions can often be put in racial and/or political contexts, and there are many examples of minority team members who have not been given appropriate credit for their contributions to science. For example, Rosalind Franklin made a crucial contribution to the discovery of the double helix structure of DNA but was not acknowledged for her contributions. There are also numerous examples of researchers exploiting vulnerable populations as study subjects, such as the Tuskegee Study, which used Black men to unethically study syphilis, as being one of the most well-known examples.14
Human research and the need for ethical review
Following the historical exploitation of vulnerable populations in research, a number of ethical codes were implemented to govern the use of human subjects in research.15 In the United States, the current policy to protect human subjects in research, termed ‘Common Rule’, is largely based on the Belmont Report.16 The Belmont Report was initially published in 1979 by the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research and was designed to promote ethical conduct of research involving human participants (see Table 6.2).
| Ethical principle | Application or action in research | Strategies for VCE programming in which research is conducted |
| Respect for persons | Individuals must be given autonomy to choose whether or not to participate in research | Provide the community or organization autonomy to participate in research Obtain informed consent from the community that clearly states research activities |
| Beneficence | Researchers must strive to do no harm or, in situations where this is not possible, researchers must maximize research benefits while minimizing possible harms | Ensure the study design is ethical, matches the mission of the community or organization, benefits as many individuals as possible, and does not involve unnecessary risks for the community Implement safeguards to protect the confidentiality of data for community members and/or organizations Interpret data in a manner that promotes good science and considers community hypotheses, perspectives, or concerns Allow the community or organization to review any description related to their group in publications or provide the opportunity for the community/organization to be anonymous |
| Justice | Risks and benefits of research should be equally distributed. In other words, researchers should only recruit subjects for reasons that are directly related to the research and should not rely on subjects because they are easily available or manipulatable | Develop research questions that support the interests of researchers and the community Agree on the expectations and responsibilities of researchers and community members Allocate study resources and credit fairly between the researchers and the community |
| Adapted from the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research.17 VCE, veterinary community engagement. | ||
To ensure concordance with the above principles, study protocols must be reviewed by an Institutional Review Board (IRB) if the investigation meets the definition of research involving human subjects, as described in 45 CFR 46.16 The U.S. Department of Health & Human Services defines research as ‘a systematic investigation, including research development, testing and evaluation, designed to develop or contribute to generalizable knowledge’. This definition encompasses data collection and analysis for scholarly activities, public health surveillance, criminal justice activities, and national security or intelligence missions. There are several exemptions to the above where research involving only minimal risk does not require a comprehensive IRB review, described further in §46.104.16
Ethical review also serves to ensure all proposed activities are scientifically sound, necessary, and justifiable in their use of resources. The process provides researchers with an independent expert review of the study aims, design, and methodology, and helps to identify potential risks before they are realized. Particularly for vulnerable populations of people (e.g. children, youth, historically marginalized and people with disabilities), IRB review can be thought of as a minimum standard and additional ethical safeguards may be needed.
Animal research and the need for ethical review
Laws governing the ethical use of animals in research are sparse compared with human research and differ worldwide. In the United States, the first legislation related to the use of animals in research was introduced in 1966, entitled the Animal Welfare Act, which remains the primary legislation enforced today. The act provides general standards for the humane treatment of animals that are bred for commercial or Internet sales, used in biomedical research, or transported commercially.18
A key requirement of the Animal Welfare Act stipulates that research facilities must appoint an Institutional Animal Care and Use Committee (IACUC) to monitor the use and care of animals at the facility. The IACUC is also tasked with reviewing and approving all proposed activities involving animals to ensure they do not unnecessarily duplicate previous research or cause unnecessary pain, discomfort, and distress. The committee must include a chairman and at least two other members, including a Doctor of Veterinary Medicine and an individual who is not affiliated with the facility.18
It is important to note that the regulations outlined in the Animal Welfare Act do not directly address research or training involving privately owned animals, although ethical review is crucially important to protect animal welfare and promote good science. Many research institutions therefore require that all studies undergo IACUC review. The need for ethical review can present a challenge for individuals from organizations without established IACUC committees, so many partner with academic institutions or rely on sponsors for ethical review.19
Activities involving privately owned animals also require additional ethical considerations that are not covered by the IACUC review. For example, informed consent is a key component in the ethical conduct of research, and many journals will require proof of owner-informed consent as well as an IACUC review for publication. Researchers may also consider the principle of justice, described in the Belmont Report,17 when recruiting pets to participate in research. That is to say, researchers should not recruit vulnerable animal populations (e.g. shelter animals, pets from underserved areas) simply because they are accessible but must also consider whether the research or training has potential benefits for these populations as well as the potential for harm. Researchers must also ensure that an individual’s refusal to participate in research does not preclude their animals from receiving care.
Training in human and animal ethics
A key requirement of the human ethical review process necessitates that all personnel including investigators, study contacts, students and any staff involved in research are appropriately trained in the ethical conduct of research whether they are associated with a university or not. As a result, community partners and collaborators involved in VCE research will often be required to complete a human research training program. Many institutions rely on third-party human ethics training programs, such as the Collaborative Institutional Training Initiative (CITI), to fulfill these requirements.
Individuals involved in the care or use of animals in research must also undergo training, as stipulated in the Animal Welfare Act.18 The training should include information related to the humane care and use of animals, the use of research methodologies that minimize animal pain or discomfort, the protocols to report deficiencies in animal care, and the availability of the Animal Welfare Information Center for information related to the use of animals in research, testing, and teaching.18
Suggestions for ethical engagement in CBPR
CBPR entails ethical challenges that arise from balancing community and scientific interests. Following scientific norms can be difficult when collaborating with organizations whose interests are directly impacted by the study findings. The ethical review process can also inadvertently place communities at risk, as IRBs are primarily concerned with protecting the rights of individual human subjects in research, rather than communities or organizations.20 Researchers and communities should therefore implement strategies to protect themselves throughout the research process, as detailed in Table 6.2.
A key method to protect community members and set the expectations of both parties is to develop and enter a formal, written agreement before the study begins. The agreement should outline matters related to data ownership, storage, and sharing. Some organizations, for example, may not be willing to share their dataset in a public repository for secondary analysis, meaning the researchers would need to seek an exemption if data sharing was required by scientific journals. The agreement should also clarify how issues related to the publication of research findings will be handled, including the timeline for publication, expectations for authorship, responsibilities for drafting and revising manuscripts, and plans for widespread dissemination of findings, including press releases. It is particularly important to clarify how research findings will be published in situations where data may depict the community in a negative light, which is oftentimes through the removal of identifying information prior to publication.21
Overcoming differences between researchers and communities in CBPR
A multitude of differences can exist between researchers and communities that may jeopardize the research process, including cultural or language differences, as well as differences in research expectations and priorities. Researchers must be cognizant of any potential differences, particularly if they may lead to a power imbalance, and implement strategies to mitigate such inequities.
One example relates to researchers’ need to balance the demands of an academic career with the priorities of community partners. Developing community relationships is a time-consuming process, especially when working with communities that have been subject to historical exploitation. During this process, researchers may need to participate in community events and projects beyond the scope of the research itself. It is therefore important that researchers recognize the time constraints of CBPR prior to undertaking projects. In situations where researchers need to rapidly publish findings and/or acquire funding, it may be advisable to concurrently pursue smaller community-based projects while developing a larger CBPR study.22 Ultimately, academic institutions also need to recognize the differences between community-based research and traditional approaches when considering faculty members’ research output.23
The use of resources in CBPR is another important consideration. Funding is necessary to allow researchers and communities to establish partnerships and develop trust through regular communication and meetings, to provide community training, to support project management and data collection, and to aid research dissemination. In many cases, researchers control the grant funds and are responsible for reporting to funding organizations. To manage resources fairly, researchers and community members should clearly define their roles at the start of the project, communicate openly throughout the project, and share decision-making related to money and resources.23,24
A final example pertains to the preparation of grant proposals and manuscripts. University partners are often more familiar with the idiosyncrasies of research proposals and publications and may take the lead when preparing such documents. However, community partners must be afforded the opportunity to contribute, which should include authorship when appropriate. To achieve this, researchers may need to adopt longer timelines than usual to provide the community with sufficient time to revise the documents. Researchers may need to use multiple communication strategies, such as face-to-face meetings, email, and telephone, to ensure community partners can provide their perspectives1 and should consider disseminating information to the community through additional avenues beyond scientific publications, such as infographics, news media, social media, and community newsletters.
Conclusion
Research, including program evaluation, is an essential component to the success of VCE programs. However, research and evaluation must be conducted ethically with the interests of the community, and interested parties placed at the forefront. True partnerships exist when community leaders have input and even direct research inquiry. A process for community members to contribute to the design and implementation of the project should be established and guidelines for ethical review must be strictly followed. Communication between research teams, programs and community partners, and citizens should be clear and transparent. Finally, results should be shared with all interested parties.
References
| 1. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 2. | Koh HK. Leadership in public health. J Cancer Educ. 2009;24:S11–S18. doi: 10.1007/BF03182303 |
| 3. | Federal Emergency Management Agency (FEMA). Comprehensive Preparedness Guide 101: Developing and Maintaining Emergency Operations Plans. https://www.fema.gov/sites/default/files/2020-05/CPG_101_V2_30NOV2010_FINAL_508.pdf. Accessed August 24, 2023. |
| 4. | Arends R. Learning to Teach. 6th ed. McGraw-Hill; 2004. |
| 5. | Burns A. Doing Action Research in English Language Teaching: A Guide for Practitioners. Routledge; 2009. |
| 6. | Green S, Johnson R. Assessment Is Essential. 1st ed. McGraw-Hill Higher Education; 2009. |
| 7. | Creswell JW. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. 2nd ed. SAGE Publications; 2003. |
| 8. | Rubin CL, Martinez LS, Chu J, et al. Community-engaged pedagogy: a strengths-based approach to involving diverse stakeholders in research partnerships. Prog Community Health Partnersh. 2012;6(4):481–490. doi: 10.1353/cpr.2012.0057 |
| 9. | Rycroft-Malone J, Bucknall T. Models and Frameworks for Implementing Evidence-Based Practice: Linking Evidence to Action. John Wiley & Sons; 2010. |
| 10. | Evidence-Based Veterinary Medicine Association (EBVMA). What Is Evidence-Based Medicine? https://www.ebvma.org/. Accessed April 13, 2023. |
| 11. | Silvertown J. A new dawn for citizen science. Trends Ecol Evol. 2009;24(9):467–471. doi: 10.1016/j.tree.2009.03.017 |
| 12. | The Association for Qualitative Research (AQR). https://www.aqr.org.uk/. Accessed April 7, 2023. |
| 13. | Israel BA, Schulz AJ, Parker EA, Becker AB. Review of community-based research: assessing partnership approaches to improve public health. Ann Rev Public Health. 1998;19(1):173–202. doi: 10.1146/annurev.publhealth.19.1.173 |
| 14. | Brandt AM. Racism and Research: The Case of the Tuskegee Syphilis Study. Hastings Center Report. 1978:21–29. |
| 15. | Rice TW. The historical, ethical, and legal background of human-subjects research. Respir Care. 2008;53(10):1325–1329. |
| 16. | United States Department of Health and Human Services. Code of Federal Regulations: Title 45, Public Welfare; Part 46, Protection of Human Subjects. 2018. https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html. Accessed August 29, 2022. |
| 17. | National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research. 1979. https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/read-the-belmont-report/index.html. Accessed August 29, 2022. |
| 18. | United States Department of Agriculture (USDA). Animal Welfare Act and Animal Welfare Regulations. https://www.aphis.usda.gov/animal_welfare/downloads/AC_BlueBook_AWA_508_comp_version.pdf. Accessed August 24, 2023. |
| 19. | Bertout JA, Baneux PJR, Robertson-Plouch CK. Recommendations for ethical review of veterinary clinical trials. Front Vet Sci. 2021;8:715926. doi: 10.3389/fvets.2021.715926 |
| 20. | Flicker S, Travers R, Guta A, McDonald S, Meagher A. Ethical dilemmas in community-based participatory research: recommendations for institutional review boards. J Urban Health. 2007;84(4):478–493. doi: 10.1007/s11524-007-9165-7 |
| 21. | Resnik DB, Kennedy CE. Balancing scientific and community interests in community-based participatory research. Account Res. 2010;17(4):198–210. doi: 10.1080/08989621.2010.493095 |
| 22. | D’Alonzo KT. Getting started in CBPR: lessons in building community partnerships for new researchers. Nurs Inquiry. 2010;17(4):282–288. doi: 10.1111/j.1440-1800.2010.00510.x |
| 23. | Kennedy C, Vogel A, Goldberg-Freeman C, Kass N, Farfel M. Faculty perspectives on community-based research: ‘I see this still as a journey’. J Empir Res Hum Res Ethics. 2009;4(2):3–16. doi: 10.1525/jer.2009.4.2.3 |
| 24. | Strickland CJ. Challenges in community-based participatory research implementation: experiences in cancer prevention with Pacific Northwest American Indian tribes. Cancer Control. 2006;13(3):230–236. doi: 10.1177/107327480601300312 |
Short summary
These Principles of VCE are closely adapted from the 2nd Edition of the Principles of Community Engagement, published by a coalition of human health agencies to guide human healthcare programs. This publication echoes their original nine principles but has been reorganized and refined to focus on programs providing healthcare services to animals.
When engaging with the animals and families in marginalized, underserved, or underrepresented communities, the veterinary medical field has opportunities and responsibilities. Project volunteers are often excited and passionate, and if guided well, their efforts can have significant impacts on people and their animals. Unfortunately, good intentions do not guarantee positive outcomes. The goal of the document is to enhance understanding of the challenges in designing, implementing, and sustaining VCE programs, and to ensure the dignity, health, and welfare of animals and the communities caring for them.
Our field has an obligation to identify and follow evidence-based ethical engagement practices refined through decades of research from human health engagement programs. As VCE continues to gain momentum in academic and research settings, the public sector, philanthropic organizations, and veterinary student training programs, formal guidelines for such engagement have become necessary.
Appendix A: Glossary of terms
A note about the glossary and its use:
The terms included here are those the authors felt would be useful to explain more fully in this document and appear as bolded terms throughout the document. Some of these entries are intended as definitions, while others are comments to clarify use in a specific context. We acknowledge that many of these terms have multiple definitions or, in fact, may not have been previously defined. The intent is to add clarity to the document. Preferred terminology may evolve over time and will be updated as appropriate. Citations or links to further information for each term are provided when available and may also evolve over time.
| Term | Chapter Bolded | Definition or Note |
| Access to Veterinary Care/Accessible Veterinary Care (AVC) | 4 | Accessible Veterinary Care is an approach to advancing the vision that all companion animals deserve access to regular veterinary care regardless of the circumstances in which they or their families live. AVC is an emerging discipline in veterinary medicine in the United States and represents a paradigm shift for an industry that historically relied solely on fee for service. The origins of this movement can in part be traced to the Access to Care Coalition which published a report on the matter in 2018, although several other institutions within academia, animal welfare, and the for-profit sector have been working on the issue for more than a decade, with many practitioners employing these techniques for decades. See the following references for more information.1–3 |
| Animal-assisted healthcare | ES | A component of healthcare that incorporates therapy animals to improve the physical and mental health of [human] patients with certain acute or chronic diseases. Sometimes called pet-facilitated therapy, although animal-assisted activities is the preferred term.4 |
| Animal welfare | 1 | Animal welfare refers to how an animal is coping with the conditions in which it lives. An animal is in a good state of welfare if (as indicated by scientific deduction and direct observation) it is healthy, comfortable, well-nourished, safe, able to express innate behaviors, and if it is not suffering from unpleasant states such as pain, fear, and distress. The term ‘animal welfare industry’ is used to describe a collection of various humane and animal sheltering organizations. This industry is made up of ‘animal welfare organizations’ dedicated to advancing animal welfare in many different ways (most commonly companion animals but sometimes other species as well).5 Welfare industry organizations include but are not limited to municipal and privately-run animal shelters, non-profit or hybrid animal rescue and shelter organizations, and also national animal welfare-focused organizations that fund and facilitate but may not directly house or care for animals. |
| Animal Welfare Act of 1966 | 6 | One of the most important federal laws regarding animals in the United States. The Animal Welfare Act (AWA) was first passed in 1966 in response to several highly publicized incidents of pet dogs ending up in research laboratories. The AWA charges the USDA with enforcing standards of humane care for animals bred for commercial use or Internet sales, used in biomedical research, exhibited, or transported commercially across state lines. The Animal Plant Health Inspection Service (APHIS) administers the AWA. The AWA establishes requirements concerning the transportation, sale, and handling of certain animals and includes restrictions on the importation of live dogs for purposes of resale, prohibitions on animal fighting ventures, and provisions intended to prevent the theft of personal pets.6 |
| Asset-based ideology, community-driven approach | 2 | ‘Asset-based approaches value the capacity, skills and knowledge and connections in individuals and communities. They focus on the positive capacity of individuals and communities rather than solely on their needs, deficits, and problems’.7 Also referred to as ‘strength-based’ approach. |
| Authentic representation | 1 | In the context of community engagement: communication and behavior between organizations and community members that demonstrate transparent collaboration in content (message), source (people), and process.8 |
| Beneficence/non-maleficence | 1 | In human medical ethics: Beneficence: Doing good or acting in the best interest of the patient; altruism; contextual moral obligation. Non-maleficence: obligation to act in ways that do not inflict harm. ‘maximum primum non nocere’ (first do no harm). Closely related terms but not the same; there may be some things that are value-neutral for the patient.9 |
| Capacity for care (C4C) | 4 | Capacity for care (C4C), considered holistically, means the ability to meet the needs of every animal admitted to an animal shelter, regardless of how they came in, when they came in, or their age, health status and personality. Every sheltering organization has a C4C and must function within it to allow them to be the best resource for the animals and people in their shelter and community.10 |
| Citizen science | 6 | Projects that incorporate community volunteers who collect and/or process data as part of a scientific inquiry.11 |
| Collective self-determination | 2 | A concept that considers an individual’s autonomy and right to freely determine their political status and economic, social, and cultural development, but in collective terms as it relates to participation in building group identity.12 |
| Community | 1 | Relationships representing shared geographic, value-based and cultural systems while providing for individual differences.13 |
| Community-based participatory research (CBPR) | 6 | As defined by NIH, research in public health focused on social, structural, and physical environmental inequities through the active involvement of community members, organizational representatives, and researchers in all aspects of the research process.14 |
| Contextualized care | 1 | Adaptation of evidence-based medicine to the real-life constraints and opportunities existing in a given family or community.15 |
| Cultural humility | 1 | In the context of healthcare, cultural humility incorporates a lifelong commitment to self-evaluation and self-critique, to redressing the power imbalances in the patient-physician dynamic, and to developing mutually beneficial and non-paternalistic clinical and advocacy partnerships with communities on behalf of individuals and defined populations.16,17 |
| Culturally responsive care | 1 | Care provision approach that recognizes and values all aspects of an individual’s identity. In veterinary medicine, it takes the families that patients live within into context.18 |
| Effective care | 1 | In human medicine, ‘effective care’ refers to services that are of proven value and have no significant tradeoffs – that is, the benefits of the services so far outweigh the risks that all patients with specific medical needs should receive them.19 |
| Empowerment-based evaluation | 6 | The use of evaluation concepts, techniques, and findings to foster improvement and self-determination. Program interested parties, including community members and clients, construct and conduct their own evaluations, which can be facilitated by an outside expert.13,20 |
| Evidence-based (veterinary) medicine | 6 | The formal strategy to integrate the best research evidence available combined with clinical expertise as well as the unique needs or wishes of each patient/client in clinical practice decision-making.21 |
| Experimental research | 6 | A type of research design which is aimed at determining if a cause-effect relationship exists between one factor or a set of factors, the independent variable(s), and a second factor or set of factors, the dependent variables. The researcher takes control of and manipulates the independent variable, usually by randomly assigning participants to two or more different groups that receive different treatments or implementations of the independent variable.22,23 |
| Family Quality of Life (FQoL) | 3 | A dynamic sense of well-being of the family, collectively and subjectively defined and informed by its members, in which individual and family-level needs interact. The most unique characteristic of FQoL is the emphasis on examining the perceptions and dynamics of the family unit as a whole. There are numerous assessment tools available for use in various contexts.24 |
| Fear Free ®, LLC/Low Stress Handling ® | 1 | Online education systems that offer various training certificates on animal body language, humane handling techniques, emotional well-being, enrichment, and reduction of fear, anxiety, and stress in pets with a focus on improving the experience of humans and pets in companion animal veterinary practice.25,26 These concepts can be applied to animal interactions in all settings, and one need not be certified to implement these concepts in animal interactions. |
| Five Freedoms/Five Domains | 1 | The Five Freedoms were originally defined by the Brambell report in 1965 with regard to farm animal welfare.27 They have been updated and adapted many times since28 and have been the basis for many animal welfare guidelines such as the Association of Shelter Veterinarians Guidelines for Standards of Care in Animal Shelters.29 The Five Domains (listed in parentheses) are a more modern iteration of the Five Freedoms developed by Mellor et al. that place additional emphasis on creating positive experiences as well as avoiding negative experiences in order to optimize welfare30 as well as a summative overall welfare state. Freedom from hunger and thirst (Nutrition) Freedom from discomfort (Environment and Enrichment) Freedom from pain/injury/disease (Health) Freedom to express species-specific behavior (Behavior) Freedom from fear and distress (Mental state) |
| Hidden curriculum | 3 | Refers to the unwritten, unofficial, and often unintended lessons, values, and perspectives that students learn in school.31 |
| Human-animal bond | 1 | A mutually beneficial and dynamic relationship between people and animals that is influenced by behaviors that are essential to the health and well-being of both. This includes but is not limited to, emotional, psychological, and physical interactions with people, animals, and the environment.32 |
| Informed consent | 1 | The process by which an individual, pet owner, or authorized party is informed of the purpose, procedures, risks, and benefits of a research study and gives written or oral authorization for their participation in the study, as required for the protection of subjects in research.33 The AVMA recommends the use of the term ‘owner consent’ rather than ‘informed consent’ when describing the process of detailing the risks, benefits, and alternatives of a given medical procedure and obtaining written authorization for the clinical treatment or procedure in matters relating to veterinary medicine.34 |
| Institutional Animal Care and Use Committee (IACUC) | 6 | A stipulation of the Animal Welfare Act that states that research facilities must appoint this committee to monitor the use and care of animals at and/or owned by that facility (see § 2.31 in6). |
| See Chapter 6 for more details on the composition of this committee’s members. | ||
| Institutional Review Board (IRB) | 6 | Under FDA regulations, an Institutional Review Board is a group that has been formally designated to review and monitor biomedical research involving human subjects. An IRB has the authority to approve, require modifications in (to secure approval), or disapprove research. This group review serves to protect the rights and welfare of human research subjects.35 |
| Interdisciplinary collaboration | 1 | In healthcare, ‘collaboration’ is defined as a complex phenomenon that brings together two or more individuals, often from different professional disciplines (interdisciplinary), who work to achieve shared aims and objectives which often can result in improved outcomes for patients. This concept applies to the relationship that works between different types of healthcare and non-healthcare organizations. This phenomenon is also seen in One Health initiatives where veterinary and human providers work to improve outcomes for all recipients.36 |
| Interested parties | 1 | May include animals, animal caretakers, owners, organizations, and individuals who contribute to or are directly or indirectly impacted by program components or activities, and students or investigators benefiting from education or research data through VCE programming. Can be used for any tie groups or individuals impacted by actions. Used interchangeably in this document for the term ‘stakeholders’, a term often used in business relationships but which has colonialist roots and emphasizes those with power in a relationship. |
| Justice | 1 | ‘The principle of justice in medical ethics refers to a fair and equitable distribution of health resources’.37 |
| Least harms approach | 1 | Provides care that alleviates distress or suffering even when the medical or behavioral problem may persist, the diagnosis may go unconfirmed, or owner compliance may be uncertain. This approach includes providing only necessary interventions with attention to least intrusive minimally aversive (LIMA) principles.38 |
| Memorandum of Understanding (MOU) | 4 | A statement of intent between participating organizations to work together and often states goals, objectives, or the purpose for the partnership, details the terms of and conditions for the agreement, and outlines the operations needed to achieve the goals or purpose.39 |
| Mission creep | 4 | The phenomenon is when an organization takes on new activities that lie slightly outside its core focus. When this process is ongoing, efforts and resources can move in this direction and cause the organization’s outcomes to shift. A common reason for mission creep occurs when funding is scarce and organizations ‘follow the money’ from available sources that do not share an aligned mission. When this process occurs unintentionally or without reflection, there can be negative effects on a program, its outcomes, and stakeholders.40 |
| Mixed-methods research | 6 | An approach to knowledge (theory and practice) that attempts to consider multiple viewpoints, perspectives, and positions, including the standpoints of qualitative and quantitative research.41 |
| Needs assessment | 1 | A structured inquiry (diagnostic process) at the level of the community that helps project leaders and community members identify gaps in animal health services or resources in their community while also assessing strengths and assets. It is a collaborative process to determine and negotiate future actions.42 |
| Non-experimental research | 6 | Research that lacks manipulation of an independent variable. Variables of interest are measured as they naturally occur in the lab or the real world.43 |
| One Health | 1 | The mutual relationship between people, animals, and the environment acknowledges that the health of each has positive or negative impacts on the health of all.44 |
| One Welfare | 1 | The interconnections between animal welfare, human well-being, and their physical and social environment.45,46 |
| Pain scale | 1 | Scales are used to assess the level of pain in animals. The pain scale allows a more objective assessment of a subjective pain state by and between an observer(s).47–49 |
| Patient and family-centered care | 3 | In human medicine, patient- and family-centered care encourages active collaboration and shared decision-making between patients, families, and providers to design and manage a customized and comprehensive care plan. Considerations include not only clinical perspectives but also an emotional, mental, spiritual, social, and financial perspectives.50 |
| Privilege | 3 | ‘Privilege’ in a social context, refers to certain social advantages, benefits, or degrees of prestige and respect that an individual has by virtue of belonging to certain social identity groups. Within American and other Western societies, these privileged social identities – of people who have historically occupied positions of dominance over others – include whites, males, heterosexuals, Christians, and the wealthy, among others.51 |
| Programmatic evaluation | 1 | Methods of assessment of a program which may include surveying the community leaders, members, or pet owners, assessing a community’s animal population for health markers along with anthropological, sociological, epidemiological, participatory or other types of methodologies. |
| Public health | 1 | Public health is the science of protecting and improving the health of people and their communities. This work is achieved by promoting healthy lifestyles, researching disease and injury prevention, and detecting, preventing, and responding to infectious diseases. Overall, public health is concerned with protecting the health of entire populations. These populations can be as small as a local neighborhood or as big as an entire country or region of the world.52 |
| Qualitative research | 6 | Exploratory, often narrative-based data that aim to improve understanding of a concept or experience through documentation of personal experiences or perceptions. Often methods can be based on survey, interview or focus group data, along with literature reviews, direct observation and scientific descriptions of individual peoples and cultures.53 |
| Quality of life (QoL) assessment | 1 | QoL aims to identify aspects of the animal’s life that are important for it as an individual, this may be different or encompass more issues than are considered by the healthcare professional where the primary focus may be a specific health-related outcome. QoL assessments aim to provide an all-encompassing evaluation of animal welfare. In comparison to more limited, disease-focused welfare assessments, they have the potential to better identify welfare deficiencies, allowing veterinarians to target improvement strategies for greater benefit.54,55 |
| Quantitative research | 6 | Scientific exploration and explanation that is numerically based and data point driven. Statistical and mathematical analyses/descriptions of a research issue or question that can often be displayed numerically or graphically.56 |
| Scope of services/care | 1 | The breadth and depth of services or care provided by a program or initiative. This is part of practice transparency and considers many factors including finances and sustainability, among others. |
| Social determinants of health | 1 | Social determinants of health are the conditions in which people are born, grow, live, work, and age. They include factors such as socioeconomic status, education, neighborhood and physical environment, employment, and social support networks, as well as access to healthcare.57 |
| Spectrum of care | 1 | All evidence-supported diagnostic testing and treatment options are filtered through the lens of the specific circumstances of the pet and owner to select the option considered most acceptable based on the owner’s expectations and financial considerations. Care options should be periodically reviewed.58 |
| Underrepresented/ marginalized/ underserved | ES | With respect to healthcare, underrepresented and marginalized populations include people who experience discrimination of any kind and encounter barriers (e.g. racial, ethnic, gender, sexual orientation, economic, cultural, and/or linguistic) to accessing public health and healthcare goods and services. Underserved populations are ones that are disadvantaged in relation to other groups because of structural/societal obstacles and disparities.59 |
| Veterinary | ES | Scope of use in this document: as an adjective relating to activities that treat or prevent diseases or injuries of animals vs an activity that is animal-related but does not legally require action or oversight by a licensed veterinarian. |
| Veterinary community engagement (VCE) | ES | The process of working in collaboration with communities to provide veterinary medical services that impact the health and well-being of animals and the communities of humans that care for them. |
| NESCMC, 2023 based on ‘community engagement’ as defined by CDC, 1997, first edition of parent CDC document.60 | ||
| Veterinary professionals | 1 | In this document: relating to persons who treat or prevent diseases or injuries of animals typically while working in a healthcare setting. This term can apply to licensed veterinarians who can diagnose medical conditions and prescribe treatment and paraprofessional staff such as credentialed veterinary technicians, and non-credentialed technicians or veterinary assistants who assist veterinarians in their work. |
| Volunteerism | 3 | Volunteerism is defined by Wilson as ‘any activity in which time is given freely to benefit another person, group, or organization’.61 Using volunteers for programming and care delivery is not inherently negative. Volunteerism can cause harm when the priority is put on the volunteer experience over the goals and outcomes most important and relevant to the communities involved.61,62 |
References
| 1. | Program for Pet Health Equity. Access to Veterinary Care Coalition (AVCC). https://pphe.utk.edu/access-to-veterinary-care-coalition-avcc/. Accessed August 14, 2023. |
| 2. | ASPCApro. Access to Veterinary Care Resources. https://www.aspcapro.org/access-veterinary-care-resources. Accessed August 14, 2023. |
| 3. | The Veterinary Care Accessibility Project. https://www.accesstovetcare.org/. Accessed August 14, 2023. |
| 4. | National Cancer Institute. NCI Dictionaries. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/animal-assisted-therapy/. Accessed June 30, 2023. |
| 5. | American Veterinary Medical Association (AVMA). Animal Welfare: What Is It? https://www.avma.org/resources/animal-health-welfare/animal-welfare-what-it. Accessed August 15, 2023. |
| 6. | United States Department of Agriculture (USDA). Animal Welfare Act and Animal Welfare Regulations. https://www.aphis.usda.gov/animal_welfare/downloads/AC_BlueBook_AWA_508_comp_version.pdf. Accessed August 24, 2023. |
| 7. | McLean J. Asset Based Approaches for Health Improvement: Redressing the Balance. Glasgow Centre for Population Health; 2011. https://www.gcph.co.uk/assets/0000/2627/GCPH_Briefing_Paper_CS9web.pdf. Accessed August 24, 2023. |
| 8. | Johnston KA, Lane AB. An authenticity matrix for community engagement. Public Relat Rev. 2019;45(4):101811. doi: 10.1016/j.pubrev.2019.101811 |
| 9. | Varkey B. Principles of clinical ethics and their application to practice. Med Principles Pract. 2021;30(1):17–28. doi: 10.1159/000509119 |
| 10. | UC Davis Koret Shelter Medicine Program. Overview of Capacity for Care (C4C). https://www.sheltermedicine.com/library/resources/?r=overview-of-capacity-for-care-c4c. Accessed August 15, 2023. |
| 11. | Silvertown J. A new dawn for citizen science. Trends Ecol Evol. 2009;24(9):467–471. doi: 10.1016/j.tree.2009.03.017 |
| 12. | Thomas EF, Amiot CE, Louis WR, Goddard A. Collective self-determination: how the agent of help promotes pride, well-being, and support for intergroup helping. Personal Soc Psychol Bull. 2017;43(5):662–677. doi: 10.1177/0146167217695553 |
| 13. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
| 14. | Israel BA, Schulz AJ, Parker EA, Becker AB. Review of community-based research: assessing partnership approaches to improve public health. Ann Rev Public Health. 1998;19(1):173–202. doi: 10.1146/annurev.publhealth.19.1.173 |
| 15. | Weiner SJ. Contextualizing care: an essential and measurable clinical competency. Patient Educ Counsel. 2022;105(3):594–598. doi: 10.1016/j.pec.2021.06.016 |
| 16. | Tervalon M, Murray-Garcia J. Cultural humility versus cultural competence: a critical distinction in defining physician training outcomes in multicultural education. J Health Care Poor Underserv. 1998;9(2):117–125. doi: 10.1353/hpu.2010.0233 |
| 17. | Foronda C. A theory of cultural humility. J Transcult Nurs. 2020;31(1):7–12. doi: 10.1177/1043659619875184 |
| 18. | Minnesota Department of Health. Culturally Responsive Care. https://www.health.state.mn.us/docs/communities/titlev/cultresponsive.pdf. Accessed August 24, 2023. |
| 19. | Wennberg JE. Effective Care: A Dartmouth Atlas Project Topic Brief. The Dartmouth Institute for Health Policy and Clinical Practice; 2007. https://www.ncbi.nlm.nih.gov/books/NBK586630/. Accessed August 24, 2023. |
| 20. | Fetterman DM. 2001 INVITED ADDRESS: empowerment evaluation: building communities of practice and a culture of learning. Am J Commun Psychol. 2002;30(1):89–102. doi: 10.1023/A:1014324218388 |
| 21. | Evidence-Based Veterinary Medicine Association (EBVMA). What Is Evidence-Based Medicine? https://www.ebvma.org/. Accessed April 13, 2023. |
| 22. | Cook TD, Campbell DT, Day A. Quasi-Experimentation: Design & Analysis Issues for Field Settings. Houghton Mifflin; 1979. |
| 23. | Ellis TJ, Levy Y. Towards a guide for novice researchers on research methodology: review and proposed methods. Issues Inform Sci Inform Technol. 2009;6:323–337. doi: 10.28945/1062 |
| 24. | Hu X, Summers J, Turnbull A, Zuna N. The quantitative measurement of family quality of life: a review of available instruments. J Intellect Disab Res. 2011;55(12):1098–1114. doi: 10.1111/j.1365-2788.2011.01463.x |
| 25. | Cattle Dog Publishing. What Is Low Stress Handling? https://cattledogpublishing.com/why-and-what-is-low-stress-handling/. Accessed April 13, 2023. |
| 26. | Fear Free. What is fear free? https://fearfreepets.com/about/what-is-fear-free/. Accessed August 15, 2023. |
| 27. | Brambell F. Report of the Technical Committee to Enquire into the Welfare of Livestock Kept Under Intensive Conditions. Her Majesty’s Stationery Office; 1965. |
| 28. | Farm Animal Welfare Council. Farm Animal Welfare in Great BritaIn: Past, Present and Future. Department for Environment, Food & Rural Affairs; 2009. |
| 29. | The Association of Shelter Veterinarians (ASV). The guidelines for standards of care in animal shelters: second edition. J Shelter Med Community Animal Health. 2022;1:1–76. doi: 10.56771/ASVguidelines.2022 |
| 30. | Mellor DJ, Beausoleil NJ, Littlewood KE, McLean AN, McGreevy PD, Jones B, et al. The 2020 five domains model: including human–animal interactions in assessments of animal welfare. Animals. 2020;10(10):1870. doi: 10.3390/ani10101870 |
| 31. | The Glossary of Education Reform. Hidden Curriculum. https://www.edglossary.org/hidden-curriculum/. Accessed August 15, 2023. |
| 32. | Human Animal Bond Research Institute (HABRI). What Is the Human-Animal Bond? https://habri.org/about/. Accessed August 15, 2023. |
| 33. | Code of Federal Regulations: Title 45, Public Welfare; Part 46, Protection of Human Subjects (US Dept of Health and Human Services). 2018. |
| 34. | Rezendes A, Kahler SC. Board Enhances AVMA Visibility. https://www.avma.org/javma-news/2007-12-15/board-enhances-avma-visibility. Accessed August 24, 2023. |
| 35. | U.S. Food & Drug Administration (FDA). Institutional Review Boards (IRBs) and Protection of Human Subjects in Clinical Trials. https://www.fda.gov/about-fda/center-drug-evaluation-and-research-cder/institutional-review-boards-irbs-and-protection-human-subjects-clinical-trials. Accessed August 15, 2023. |
| 36. | Fewster-Thuente L, Velsor-Friedrich B. Interdisciplinary collaboration for healthcare professionals. Nurs Admin Quart. 2008;32(1):40–48. doi: 10.1097/01.NAQ.0000305946.31193.61 |
| 37. | Zapata JA, Moriates C. The high-value care considerations of inpatient versus outpatient testing. AMA J Ethics. 2015;17(11):1022–1027. doi: 10.1001/journalofethics.2015.17.11.ecas1-1511 |
| 38. | Certification Council for Professional Dog Trainers (CCPDT). Least Intrusive, Minimally Aversive (LIMA) Effective Behavior Intervention Policy. https://www.ccpdt.org/about-us/least-intrusive-minimally-aversive-lima-effective-behavior-intervention-policy/. Accessed August 15, 2023. |
| 39. | Dempsey K, Pillitteri V, Regenscheid A. Managing the security of information exchanges. NIST Special Pub. 2021;800:47. doi: 10.6028/NIST.SP.800-47r1 |
| 40. | Joyce M, Szykman LR. The role of nonprofit organizations in community quality-of-life: mission creep, cherry-picking, and the sequelae of the privatization of public services. J Region Anal Policy. 2003;33(2):85–95. |
| 41. | Johnson RB, Onwuegbuzie AJ, Turner LA. Toward a definition of mixed methods research. J Mixed Methods Res. 2007;1(2):112–133. doi: 10.1177/1558689806298224 |
| 42. | Gupta K. A Practical Guide to Needs Assessment. John Wiley & Sons; 2011. |
| 43. | Price PC, Jhangiani RS, Chiang I-CA, Leighton DC, Cuttler C. Chapter 6.1: Overview of non-experimental research. In: Cuttler C, ed. Research Methods in Psychology. 3rd ed. 2017: 102–106. |
| 44. | Centers for Disease Control and Prevention (CDC). One Health. https://www.cdc.gov/onehealth/index.html. Accessed April 14, 2023. |
| 45. | Pinillos RG, Appleby MC, Manteca X, Scott-Park F, Smith C, Velarde A. One welfare – a platform for improving human and animal welfare. Vet Record. 2016;179(16):412–413. doi: 10.1136/vr.i5470 |
| 46. | One Welfare. About One Welfare. https://www.onewelfareworld.org/. Accessed April 13, 2023. |
| 47. | McCobb E. Review of Small Animal Anesthesia and Pain Management: Strategies for Success. https://www.vtvets.org/assets/docs/f6e7804c-4759-44f2-bd07-f7b2e48ebb2b.pdf. Accessed August 24, 2023. |
| 48. | Wheeler EP, Abelson AL, Paul AL, Barton BA, McCobb EC. A liposomal bupivacaine infiltrative block reduces rescue analgesia administration compared to a bupivacaine splash block after canine ovariohysterectomy in a teaching laboratory. J Am Vet Med Assoc. 2023;1(aop):1–10. doi: 10.2460/javma.23.01.0057 |
| 49. | Colorado State University. Animal Pain Scales. https://vetmedbiosci.colostate.edu/vth/services/anesthesia/animal-pain-scales/. Accessed August 15, 2023. |
| 50. | Catalyst N. What is patient-centered care? NEJM Catalyst. 2017;3(1). doi: 10.1056/CAT.17.0559 |
| 51. | García JD. Privilege (Social Inequality). Salem Press Encyclopedia; 2018. |
| 52. | CDC Foundation. What Is Public Health? https://www.cdcfoundation.org/what-public-health. Accessed August 15, 2023. |
| 53. | The Association for Qualitative Research (AQR). Qualitative Research Glossary. https://www.aqr.org.uk/glossary/. Accessed August 15, 2023. |
| 54. | Yeates J, Main D. Assessment of companion animal quality of life in veterinary practice and research. J Small Animal Pract. 2009;50(6):274–281. doi: 10.1111/j.1748-5827.2009.00755.x |
| 55. | Mullan S. Assessment of quality of life in veterinary practice: developing tools for companion animal carers and veterinarians. Vet Med. 2015;6:203–210. doi: 10.2147/VMRR.S62079 |
| 56. | Sukamolson S. Fundamentals of quantitative research. Lang Instit Chulalongkorn Univ. 2007;1(3):1–20. |
| 57. | World Health Organization (WHO). Social Determinants of Health. https://www.who.int/health-topics/social-determinants-of-health. Accessed April 7, 2023. |
| 58. | Brown CR, Garrett LD, Gilles WK, et al. Spectrum of care: more than treatment options. J Am Vet Med Assoc. 2021;259(7):712–717. doi: 10.2460/javma.259.7.712 |
| 59. | Baah FO, Teitelman AM, Riegel B. Marginalization: conceptualizing patient vulnerabilities in the framework of social determinants of health – an integrative review. Nurs Inquiry. 2019;26(1):e12268. doi: 10.1111/nin.12268 |
| 60. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 1st ed. 1997. |
| 61. | Wilson J. Volunteering. Ann Rev Sociol. 2000;26:215–240. doi: 10.1146/annurev.soc.26.1.215 |
| 62. | Adams RE, Boscarino JA. Volunteerism and well-being in the context of the World Trade Center terrorist attacks. Int J Emerg Mental Health. 2015;17(1):274. doi: 10.4172/1522-4821.1000158 |
Appendix B: List of principles of veterinary community engagement
These nine principles or pillars of veterinary community engagement (VCE) are modeled on the previously published Principles of Community Engagement.1 Although these pillars are numbered, they are not intended to be followed in a linear approach. In fact, the activities discussed in the principles should occur simultaneously and repeatedly throughout the process of developing, implementing, assessing, and continually renewing a VCE project.
Principle 1:
‘Become knowledgeable about the community’s culture, economic conditions, social networks, political and power structures, norms and values, demographic trends, history, and experience with efforts by outside groups to engage… Learn about the community’s perceptions of those initiating the engagement activities’ (p. 47).1
Principle 2:
‘Go to the community, establish relationships and build trust, work with the formal and informal leadership, and seek commitment from community organizations and leaders to create processes for mobilizing the community’ in an ethical and evidence-based way (p. 48).1
Principle 3:
Partner with the community to create change and improve community health and animal welfare (p. 50).1 Recognize how as a program leader and care provider your identity influences this partnership.
Principle 4:
‘Remember and accept that collective self-determination is the responsibility and right of all people in a community. No external entity should assume it can bestow on a community the power to act in its own self-interest’ (p. 49).1 Organizations that wish to engage a community as well as individuals seeking to effect change must be prepared to release control of actions or interventions to the community and be flexible to meet its changing needs.
Principle 5:
All aspects of community engagement must be designed to recognize and respect diversity within the community and the partnership. Acknowledge how identity impacts planning, design, and implementation (p. 51).1
Principle 6:
Be clear and transparent about the purpose or goals of the community engagement project and recognize that interested parties will come to a partnership with equally important but different goals (p. 46).1
Principle 7:
‘Community engagement can only be sustained by identifying and mobilizing community assets and strengths and by developing the community’s capacity and resources to make decisions and take action’ (p. 51).1
Principle 8:
Community collaboration requires a long-term commitment to have the best chance at a measurable and sustainable impact (p. 52).1
Principle 9:
Successful community collaboration requires continual reflection, both individually and as a group. Accountability and assessment of VCE programming are crucial for continued success.
Reference
| 1. | Centers for Disease Control and Prevention (CDC). Principles of Community Engagement. 2nd ed. 2011. https://www.atsdr.cdc.gov/communityengagement/pdf/PCE_Report_508_FINAL.pdf. Accessed August 24, 2023. |
From: Principles of Veterinary Community Engagement, 1st ed. 2024
Appendix C: Veterinary community engagement (VCE) program profiles
Introduction
As discussed at length in the main text of this document, community-engaged work is complex and challenging. At their core, VCE programs require authentically collaborative approaches to deliver veterinary services, often in resource-challenged settings. Many VCE programs also provide training or research opportunities, adding additional complexity and ethical considerations. VCE programs rely on program evaluation and assessment not only to provide insight into programmatic evolution but frequently to sustain funding and continue the work.
Methodology
A survey was created to capture operational, educational, and communication elements of program design from VCE program leads, as well as reflections on mistakes and challenges programs have faced. The survey was reviewed and approved by Institutional Review Boards at both the University of Pennsylvania (Protocol number 852211) and Cornell University (Protocol number IRB146548). Leaders of programs profiled in this section were actively recruited at the Access to Veterinary Conference in 2022 and via snowball sampling. Participants were asked to complete an online survey in June–July of 2023 (see Supplementary Materials). Information was collected via a written response or an interview at the participant’s request. Results were then compiled and edited into these program profiles. All participants provided informed consent. Participants were given an opportunity to review their program’s profile for accuracy prior to publication. They were also asked to provide an image representative of their work for which they had permission to publish.
Results
We are excited to present these program profiles as a means of illustrating VCE in action. No program can perfectly adhere to all of the principles of engagement despite the best of intentions; they were all willing to share their mistakes quite candidly. Each profile clearly demonstrates how program leaders have designed and applied principles of community engagement in the provision of veterinary services. Most programs have a teaching mission in addition to providing direct care. All integrate community members into design and decision-making when implementing their mission and vision. We felt strongly that providing these real-life examples helps make the material contained in this resource more relatable to situations faced by organizations daily. These profiles are not endorsements of programs or comprehensive in any way but selected thoughtful descriptions and examples from those on the ground.
While the editors of this document have made the creative choice to highlight programs under a particular principle, this decision is not meant to imply that a program does not also adhere to others. In most cases, several principles were employed by each program.
All participants also extended an invitation to readers to reach out to discuss their work further, particularly if elements can serve in developing other programs. Websites and contact information are included when applicable.
Principle 1: Become knowledgeable about the community you aim to serve
The Kim & Stu Lang Community Healthcare Partnership Program embodies this principle by seeking deep learning and listening from community members to understand the communities. The wisdom of the community is shared with the care teams who strive to listen with humility.
The Kim & Stu Lang Community Healthcare Partnership Program (CHPP)
Ontario Veterinary College, University of Guelph, Canada
Mission
To identify, understand and remove barriers that impede access to healthcare for companion animals, and honor the universality of the human-animal bond.
Scope of services
CHPP envisions a future where made-vulnerable humans and animals in Canada enjoy better health, stronger social support and integration into their communities, supporting the universal nature of the human-animal bond. To this end, CHPP focuses on working with three main populations: vulnerable animals in the shelter and animal welfare spaces, precariously housed people and animals, and indigenous communities within a reconciliation network. As an academic program, the scope of the work includes teaching, service, and research. Teams deploy to shelters and communities with a fully equipped MASH unit.
Program faculty have a background in social science in addition to veterinary medicine. Clinical work is enhanced through scaffolded learning encompassing social determinants of health, indigenous community history in Canada, issues of poverty and housing precarity, implicit bias training, and trauma-informed care. Fourth-year clinical rotations are tied to clinics at shelters, encampments, and subsidized housing complexes, as well as First Nations communities. In all settings, social justice, historical context, and cultural knowledge are woven throughout the experience.
CHPP works to create continual conversation among partners to ensure an iterative learning process. Participants are encouraged to occupy a ‘space of humility’ regarding the stories of others and the needs of communities. Frequent opportunities are created for community partners to provide feedback on how the project is going and identify new needs and opportunities. While primarily veterinary in nature at this time, the program is working to integrate human healthcare services into the model as they evolve.
Mistakes or challenges
Program leadership commented that they have learned a lot about budgeting and predicting what it really takes to house a new program or launch an exciting new idea. It is a precarious thing to build a budget that necessitates donations – as these vary year to year and alongside the economy, they should not be considered guarantees.

CHPP: The team on a Community Health rotation at Oneida of the Thames First Nation, including eight final-year veterinary students alongside CHPP veterinarians, interns, residents, and registered veterinary technicians.
Words of advice
‘Be humble – listen. Remain in the headspace of a “guest,” or a privileged participant who gets to figure out how to provide the requested service to the community. This may seem intuitive, but often we – as healthcare providers – come into a clinical space with an air of superiority (often unintentional): we assume to have the knowledge and it is our duty to give it to others, to tell them what is correct. If we flip the narrative to one that is community driven, it forces humility and listening for community guidance on program direction and goals.’
Information and permissions provided by:
Lynn Henderson DVM MEd CHPV, Veterinary Director of the Kim & Stu Lang Community Healthcare Partnership Program,
Principle 2: Go to the community, establish relationships and build trust, work with the formal and informal leadership, and seek commitment from community organizations and leaders to create processes for mobilizing the community.
The Community Veterinary Clinic arose from a surprising and significant gap in veterinary care made visible by a natural disaster. The ongoing programming relies on the ingenuity and resources of program leadership but also the intense commitment of community members and animal caretakers.
Community Veterinary Clinic at the Humane Society of Sonoma County (CVC at HSSC)
Santa Rosa, CA, USA
https://humanesocietysoco.org/medical-programs/community-veterinary-clinic/
Mission
To provide compassionate veterinary care in a welcoming and non-judgmental environment for low-income pet owners.
Scope of services
After the 2017 Tubbs fires in California, leadership at the Humane Society of Sonoma County (HSSC) intended to host a one-time free veterinary clinic for pet owners displaced due to the fire. They were surprised to find the clinic was instead overwhelmed by dozens of families who had never been able to receive veterinary care, disaster or not. The decision was made to pivot and to close the public, market-rate hospital already operating within HSSC. Instead, HSSC opened the Community Veterinary Clinic (CVC), a safety-net clinic to provide sliding-scale surgery, dentistry, and medical care for pets of low-income families.
The CVC is well known in the community and accepts direct calls from the public and surgical referrals from local emergency clinics, day practices, and other partners. Due to a notable scarcity of accessible surgery in the region, the clinic tackles surgeries with a good prognosis that would otherwise result in economic euthanasia or shelter surrender. The clinic also hosts a limited ‘urgent care’ medical program 1 day a week to provide care to income-qualifying families for treatable and manageable conditions.
Frontline staff field dozens of calls a day for services; they triage by urgency and ability to access care elsewhere, helping direct clients to resources. Several Spanish-speaking staff members provide care and translation as needed for Spanish-speaking clients. Because this work depends on relationships with the local community, including veterinarians, from day one, CVC leadership has worked to build relationships across all stakeholders, including clients, board members, shelter personnel and volunteers, and the greater community. By holding regular open houses and presenting at local meetings, the CVC has created a forum in which to talk about the work, share stories and enlist support.

CVC at HSSC: In response to community needs, the CVC provides subsidized medical, dentistry, and emergency surgeries, often on a referral basis from local practices. This patient is recovering from a perineal urethrostomy after presenting with a urethral obstruction referred to CVC by a partner clinic.
Mistakes or challenges
Given the clearly demonstrated need for the CVC in the community, HSSC was eager to roll out the new service. The promotional plan started with direct communication and open house presentations to private practitioners, emergency clinics, and other key referral partners to build some cushion around demand. Promotion to the public was scheduled to follow this ‘soft launch’, but a front-page story about the clinic and a banner announcing ‘Open Today, Walk-ins Welcome’ altered those plans overnight. From the start, the CVC’s staff was stretched very thin, trying to respond to public demand before a robust community support system was in place. Appointment wait times extended out 2–3 months. Expectations and communication glitches left the clinic playing catch up and tested the capacity and resilience of the small medical team.
Words of advice
‘Determine what the capacity and interest and skills are of your organization and see how that meshes with the needs in your community. In Sonoma County for instance there are already several low-cost wellness options and accessible spay/neuter services. At HSSC, we have strong anesthesia and dentistry skills and a DVM who enjoys surgery and urgent care. We also have a community with seemingly endless numbers of large dogs with pyometras and chihuahuas in heart failure and with severe dental disease. Our clinical strengths and passions help meet these care gaps in our community – saving lives and supporting families reminds us why we entered veterinary medicine and animal welfare in the first place.’
Information and permissions provided by:
Ada Norris, DVM, Community Veterinary Clinic at the Humane Society of Sonoma County,
Principle 2: Go to the community, establish relationships and build trust, work with the formal and informal leadership, and seek commitment from community members.
Project HEAL worked to develop relations in the community and promote local partnerships with local universities to advance and sustain the work and animal welfare.
Project HEAL
University of Florida (UF) College of Veterinary Medicine
Gainesville, FL, USA
https://globalhealth.med.ufl.edu/trips/project-heal/
https://www.facebook.com/groups/343280791653813
Mission
UF students and faculty collaborate with Ecuadorian veterinarians to provide for the health and well-being of the local animal populations.
Scope of services
Project HEAL was an existing program of interdisciplinary professional healthcare students at UF that did not originally include veterinary medicine but focused on human healthcare in rural and indigenous Ecuadorian villages. A veterinary student effort created a similar program for UF veterinary students in collaboration with Ecuadorian veterinary colleagues. The program provides exposure to and experiences in veterinary medicine outside of the United States in communities of low socioeconomic status with limited or no access to veterinary care.
Project HEAL is a student-run organization as well as a 1-credit elective course (VEM5506 – International Veterinary Medicine) conducted primarily in Quito, Ecuador. The course includes 4–5 preparatory wet labs that take place prior to the 10-day trip. Services include small animal preventive medicine and sterilization clinics, large animal immunization/parasite control clinics, and 2 days of cultural experiences. Clinic locations are typically managed by local contacts and veterinary partners at Universidad de las Americas. Locations are chosen based on the socioeconomic status of the community, accessibility of care and the schedule of existing local outreach programs that work in similar areas.
This course serves as an important exposure to the spectrum of care practice for veterinary students. For many, it is their first experience traveling outside of the United States, working in a field clinic environment, and encountering clients whose standard of living is well below anything they have previously witnessed. It is not unusual for students to be welcomed into clients’ homes to provide treatment, which offers a new perspective and immediate understanding of the need for and implementation of a ‘spectrum of care’ approach to veterinary care provision.

Project HEAL: After meeting their colleagues from Universidad de las Americas in Quito, Ecuador, the University of Florida students and faculty pose for a photo prior to engaging in a week-long service trip caring for small and large animals in rural Ecuadorian villages.
Mistakes or challenges
The program’s initial experiences were entirely student-led without faculty oversight of the activities in Ecuador. This led to poor student experiences, difficulty understanding the context of the work that was being done, and concerns over animal welfare which jeopardized the program’s continued existence. The inclusion of UF faculty during the on-site experiences has addressed these concerns and the program enjoys continued support from the College and the local community. Another challenge was integrating the program with the local veterinary schools and students. Working collaboratively for shared learning was a priority, though the differences in veterinary training were often too broad to overcome, which led to some (extra) challenging clinical experiences and damaged relationships. A formal written MOU between the universities formalizing the partnership and desire to continue to work together through Project HEAL and other initiatives has been mutually beneficial.
Impact
‘This partnership has played a small but important part in the tremendous advancements that Ecuador has made in improving animal welfare over the last decade. There are now multiple organizations providing subsidized care in and around Quito and discussion of animal welfare concerns is widely apparent. A decade ago, it was the norm to see packs of free-roaming community dogs during our trips; while these are still present, they are smaller and fewer in between, and we are just as likely to see small breed, true “companion” animals, wearing clothing and walking on a leash with their owners.’
Information and permissions provided by:
Brian DiGangi, DVM, Clinical Associate Professor of Shelter Medicine, UF College of Veterinary Medicine, digangib@ufl.edu
Principle 3: Partner with the community to create change and improve community health and animal welfare. Recognize how as a program leader and care provider your identity influences this partnership.
Although this Kansas State University program is centered in academia, the work relies on a large, complex network of community partners who provide infrastructure and take the lead on how and where clinic services are delivered.
Shelter Medicine and Community Medicine Program
Kansas State University College of Veterinary Medicine (KSU CVM)
Manhattan, KS, USA
https://www.ksvhc.org/about/shelter-medicine/
Mission
The mission of KSU CVM is to admit to the program the next generation of veterinarians who will serve our communities here and abroad, with competence and compassion.
Scope of services
This program started as a shelter medicine program in 2014 and has expanded to deliver healthcare more broadly in the community. With more than 40 community partner organizations spanning 4 states and 2 tribal nations, the program provides access to veterinary care (AVC) and MASH events as part of an elective course. Program partners include human healthcare organizations, animal welfare groups, and veterinary organizations. The events look very different in varied locations based on the needs and work of the local community partner. Community partners provide local connections and infrastructure and enable the program to build trust and a consistent presence. Many of these liaisons are employees of affiliate organizations, although some are volunteers.
The program introduces students to populations historically not included in veterinary teaching hospitals, including clients experiencing housing insecurity, substance dependency, and those of lower socioeconomic status. The course is co-taught with a licensed social worker and focuses on communication skills and the bigger picture of veterinary medicine. The motto of the program is ‘everyone is worthy of a VCPR (vet-client-patient relationship)’, signifying that all families deserve access to veterinary care. Assessment and reflection are built into the curriculum, with student journals and time for discussion.
Because the program is centered in academia and led by a qualitative researcher, part of the work is to identify educational interventions in other affiliated disciplines, explore their applications in the veterinary space, and measure the impact of those applications.

KSU program: A primarily MASH clinic supported by a mobile unit enables the program to deploy throughout the community and work with many partners while ensuring some consistency in supplies and care delivery.
Mistakes or challenges
Program leadership has presented to professional audiences on the ‘pitfalls of community partnerships’ based on program experiences. Identifying collaborators, setting boundaries, and teaching amid the work are all challenging aspects of community-engaged work as an extension of an academic program. Leaning on partner organizations is essential but can also mean accepting slower timelines and unpredictability.
Words of advice
‘Being a part of this work has not been a linear trajectory. We had many partners ready to launch a few years ago, then COVID hit, partners changed. Ultimately the program is not going to be the model that you had on paper. Be comfortable with things evolving. Some partnerships are short term; others are long term. Community partners have their autonomy. Things will evolve. I have learned how to listen.’
Information and permissions provided by:
Ron Orchard, DVM, Community Outreach/Shelter Medicine Fellow, Kansas State University College of Veterinary Medicine,
Principle 3: Partner with the community to create change and improve community health and animal welfare. Recognize how as a program leader and care provider your identity influences this partnership.
This collaborative program relies on a strong team comprised of individuals from varied backgrounds and experiences that celebrates the diversity members bring to the table.
University of Tennessee Knoxville Shelter Medicine & The Companion Animal Initiative of Tennessee (CAIT)
Knoxville, TN, USA
https://vetmed.tennessee.edu/vmc/smallanimalhospital/sheltermedicine/
https://vetmed.tennessee.edu/outreach/cait/cait-history/
Mission
To engage in inclusive outreach and excellence in teaching to improve animal welfare and overpopulation problems in East Tennessee and beyond. To provide students with the knowledge and ability to be competent veterinarians and make a change in the communities in which they practice after graduation.
Scope of services
This collaboration between the University of Tennessee at Knoxville (UTK) Shelter Medicine team and the Companion Animal Initiative of Tennessee (CAIT) started in 2018 as the programs came together to advance both regional animal welfare and veterinary student training in the region. In partnership with 19 animal welfare organizations, the collaboration provides direct care and training in community settings, as well as an annual Animal Care and Control conference for shelter and field services professionals. Whenever possible, healthcare is delivered in concert with other organizations, including Remote Area Medical (human healthcare MASH services), humane organizations, Trap/Neuter/Vaccinate/Return clinics, or pop-up events around community celebrations.
Due to extensive community and animal welfare needs in the region, requests for clinical support overwhelm the collaboration’s ability to provide care. Ongoing efforts include strategic planning to ensure the most efficient and effective care delivery possible and to ensure requests are prioritized equitably.
Recent efforts have expanded the collaboration to include the UTK Veterinary Social Work program. Goals include a study of factors impacting the prevalence of compassion fatigue and burnout in animal welfare organizations and the creation of modules designed for animal shelter professionals to support positive mental health and well-being in these settings. Because a significant portion of the partnership is also committed to scholarship and student training, setting clear expectations on varied goals and measures of success is essential to maintaining the collaboration.
Mistakes or challenges
Measuring impact in ways that are tangible and reportable has been a weak point for the collaboration. Without robust evaluative measures in place, it is hard to gauge the impact in either the community or the training. As a program based in academia, the collaboration is reliant on a system of support based on data and evaluative measures; likewise engaged faculty need to be able to communicate the value of engaged scholarship and community-based work.

UTK-CAIT Collaboration: A mobile unit primarily designed for spay/neuter can serve as a baseline for care delivery in communities upon which collaborations and relationships develop.
Words of advice
‘We have a formal memorandum of understanding that outlines our relationships with working partners. We also meet regularly as a team to bring together the many tentacles of our work and to appreciate one another. We find creating a strong team enables us to be more equitable and respectful of partners and stakeholders – and frankly, these characteristics also define who we are as people.’
Information and permissions provided by:
Jennifer Weisent, DVM, PhD, Assistant Clinical Professor, Shelter Medicine, University of Tennessee at Knoxville, jweisent@utk.edu
Principle 4: Remember and accept that collective self-determination is the responsibility and right of all people in a community. No external entity should assume it can bestow on a community the power to act in its own self-interest. Organizations that wish to engage a community as well as individuals seeking to effect change must be prepared to release control of actions or interventions to the community and be flexible to meet its changing needs.
This partnership between the Toronto Humane Society, Grand River Veterinary Hospital, and community partners builds in robust cultural training that centers the interests and autonomy of animal caretakers.
Toronto Humane Society in partnership with Grand River Veterinary Hospital and Community Partners
Ontario, Canada
https://www.torontohumanesociety.com/
https://www.grandriverveterinaryhospital.com/
Mission
The partnership between the Toronto Humane Society (THS), Grand River Veterinary (GRVH), and Ontario communities grew from the individual work of each entity rather than an overarching organizational mission. However, over time, the collaboration has evolved to focus on keeping pets and people together and providing preventive medicine and education on issues related to public health.
Scope of services
In 2015, a spike in raccoon rabies in Southern Ontario created concern for community members and companion animals in the region. GRVH had independently begun vaccination, wellness and surgical efforts through mobile services and identified a previously unrecognized hyperendemic foci of heartworm infection. THS was engaged in receiving dogs from the area and treating rising heartworm infection rates in regional dogs. Greater collaboration between these organizations and with local partners provided infrastructure and increased community representation to more effectively deliver MASH preventive medicine and surgical clinics as requested by the community. The program relies on a network of community members to provide frontline engagement and client recruitment, as well as operational sustainability for the clinics.
Services are based, first and foremost, on needs identified by animal caretakers. For example, in some cases, dogs presenting to clinics for care are being used for breeding as a source of income for families; while both THS and GRVH are invested in increasing the provision of spay/neuter in their daily work, sterilization is not a mandatory aspect of participation. Program leaders are committed to removing barriers to accessing care but always in a way that makes it the decision of the pet owner.
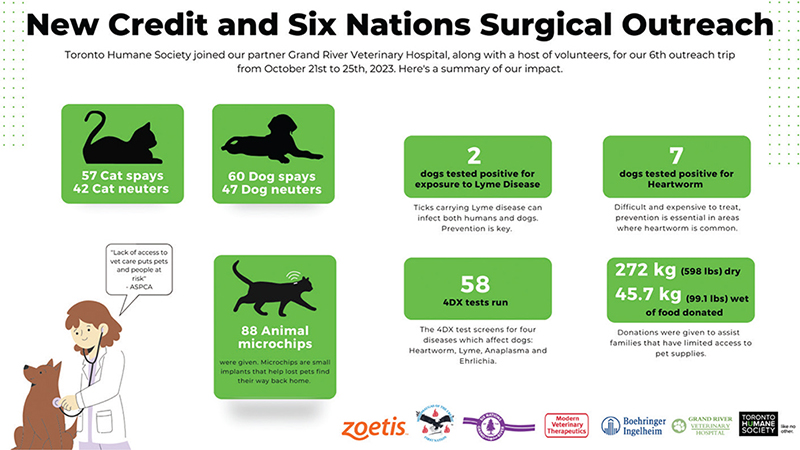
THS-GRVH: Infographics are shared with interested parties after each event to both celebrate accomplishments and plan for future programming.
Volunteer training emphasizes a judgment-free process and client autonomy. Retention of animals in the community is a priority, which can run counter to the mindset of veterinary and animal welfare professionals; checking one’s own agenda and bias prior to engaging is an important part of the process. Volunteers are also encouraged to complete a 12-week Indigenous Canada online course prior to participating in clinics. All partners prioritize improving the lives of animals and people in the community in a culturally responsible way.
Mistakes or challenges
As with all community-engaged work, communication can be challenging – especially when there are set timelines and challenging infrastructure needs. The program has had to cancel clinics when operational pieces were not in place on time. Turnover in community staff support can reduce continuity and historical knowledge of how things operate. Sometimes the line between cultural differences and individual personalities can be difficult to navigate. Overt communication is required AND needs to be done in a way that is not aggressive or disrespectful.
Words of advice
‘A really good place to start is to join an already established group that is doing it well and see what they do. It is inadvisable to leap in yourself and start something from scratch without building a better understanding of your own resources and the experiences of established successful projects. We are able to continue the work because it is done in partnership with other people and organizations. Doing it all ourselves would not be as successful.’
Information and permissions provided by:
Karen Ward, DVM, Chief Veterinary Officer,
Toronto Humane Society
Principle 5: All aspects of community engagement must be designed to recognize and respect diversity within the community and the partnership. Acknowledge how identity impacts planning, design, and implementation.
RVETS’ curriculum and training have evolved over time to develop multiple program members embedded in communities while continuing to grow volunteer experiences and ensure quality care delivery.
Rural Veterinary Experience, Teaching, and Service (RVETS)
Dixon CA, USA
Mission
The RVETS mission is to promote quality and affordable veterinary care in underserved rural areas in the United States and abroad, by providing veterinary students with practical experience and training in the medicine and surgery of horses and other animals. Further, in exposing students to the needs of these communities, we encourage future veterinarians to choose rural service as a career.
Scope of services
Since 2010, RVETS has operated annual outreach clinics to rural communities in Nicaragua, Mexico and the United States. The program was an outgrowth of Rural Area Veterinary Services (RAVS) and was started by the same founder, Dr. Eric Davis. While RAVS has maintained a small animal focus, RVETS combines their teaching mission with a focus on equid species. Working equids around the world suffer from common ailments such as dental disease, saddle sores, parasites, overpopulation, and lameness. RVETS works to provide relief from these conditions. Through training, education, and partnerships with local organizations, they develop sustainable access to veterinary medicine in the communities they serve. The goal is to provide each patient with safe, humane and high-quality medicine while providing valuable experience and training to both volunteers and community members. A core RVETS belief is that all animals deserve access to high-quality and affordable healthcare.
The scope of care includes routine and urgent care: equine castration and dentistry, lameness and hoof problems, wounds, harness sores, etc. Companion animal services are offered at some sites in Mexico and Nicaragua. Most clinics are MASH style, but the program also supports a clinic in Nicaragua which provides training, equipment, and an income for two veterinarians and maintenance personnel.
Veterinary volunteers include veterinarians, technicians, and students. An online, open access curriculum designed by a Nicaraguan vet is provided in both English and Spanish and includes not only procedures but also research and review papers. Volunteers need to complete the curriculum and practice basic techniques and are tested prior to participation.
Former students and volunteers now lead the Mexico and Nicaragua clinics and continue to provide for the ongoing training of new recruits (see NY Times article for an in-depth story on the clinic in Mexico). The program also engages in developing local paraprofessionals to continue to work in-between clinics, transferring skills to local partners. Finally, when possible, the program has connected with educational training programs in partner communities to increase opportunities for training locally (e.g. Sitting Bull College, ND).
Like other programs highlighted, the work of RVETS relies on philanthropy, including donated time by professional volunteers. Having a solid financial foundation is desirable, especially to support a stationary clinic. However, the work continues to rely on fund-raising and most of the communities RVETS serves are never going to be able to pay fees for services. A culture of philanthropy, somewhat reliable although inequitable, subsidizes the work and creates a degree of sustainability, further supported by a network of long-term volunteers and alumni.

RVETS: Adria Lessler and Tarek Isham, who at the time were UCD veterinary students, discuss the day’s clinics at the Standing Rock Reservation in North Dakota. Both are now practicing veterinarians in rural areas: Andria in California and Tarek in Montana. They are regular RVETS volunteers and have worked in the United States, Mexico, and Nicaragua.
Mistakes or challenges
Initially, the work was the thing. Leadership was focused on the delivery of care and not always connecting with people. Learning to listen to people, to see what the community really wanted and to respond to those needs, was key. Likewise, establishing local leaders in the community has been critical; spending time in the community in order to understand the underlying challenges and interpersonal dynamics strengthens the impact of the work and the partnership.
Words of advice
‘Don’t start programs until you have worked in someone else’s for a while. You don’t need to replicate their approach, but the problems and solutions are complex and you need to understand that. It is way too common for people to see an animal welfare problem and assume they can solve it rather than looking around to see how others have addressed similar problems. Gain knowledge from others, including identifying what you don’t want to do. Don’t make the same mistakes over and over and waste a lot of resources and time. This work is not a place for novice veterinarians to work unsupervised. This is NOT a place for people with questionable skills or training.’
Information and permissions provided by: Eric Davis, DVM, RVETS Co-Founder
Principle 6: Be clear and transparent about the purpose or goals of the community engagement project for all interested parties and recognize they will come to a partnership with equally important but different goals.
By staying true to their own scope and mission, Laurel’s House ensures they can sustain their part of the safety net they are working to build with other community organizations.
Laurel’s House
Houston, Texas
Mission
Laurel’s House strengthens the human-animal bond, improves public health, decreases companion animal euthanasia, and diminishes human impact on native wildlife species by providing unprecedented access to high-quality veterinary care, humane education, and rehabilitation for underserved communities, families, and species.
Scope of services
Laurel’s House is a non-profit 501c3 organization founded by veterinarians in 2019 to provide free veterinary care to families and wildlife in need in Houston, TX. Founders had observed that the sheltering systems were putting massive resources into seizing, accepting, and picking up animals with little focus on intake diversion. Given the role racial inequity can play in both humane investigations and access to veterinary care as well as investigations of animal cruelty, more widespread access to veterinary care initiatives could begin to help address this inequity.
Based on the premise that many seizures and surrenders could be prevented, the program engages in enabling pet retention through more cost-effective and humane measures including access to veterinary care and food pantry initiatives. They also work to curb free-roaming animal numbers through greater access to spay/neuter.
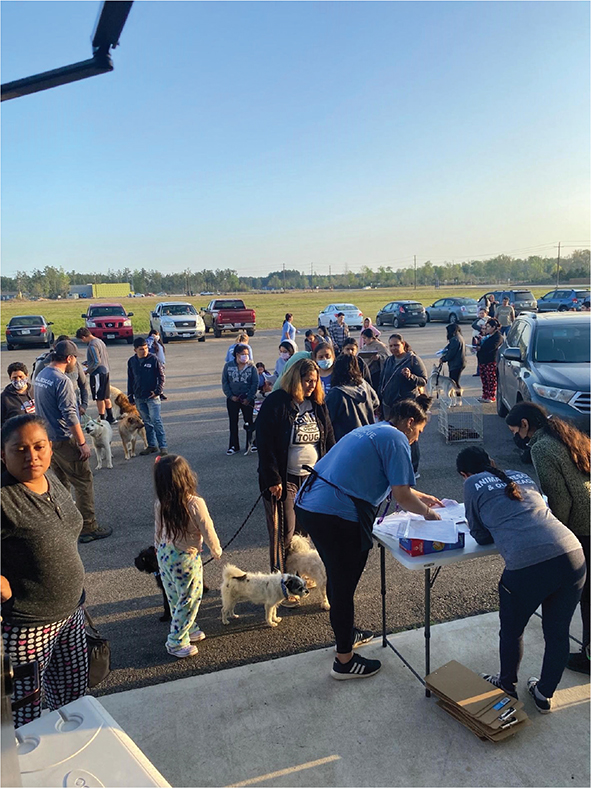
Laurel’s House: Families line up with their pets to access spay/neuter surgery and preventive care at no cost through Laurel’s House.
Maintaining a conversational, non-judgmental approach with clients and the community is a foundational principle for Laurel’s House. Likewise, client needs are not based on perception but on inquiry, employing an asset-based approach to the provision of care. Additionally, partnerships include others working in animal welfare and human support services. Clients are referred to the clinic by local shelters, humane investigators, social workers, or veterinarians working in local private clinics. Active website interactions and social media posting promote the program to community members who self-identify as needing the care provided at Laurel’s House.
Mistakes or challenges
‘Initially it was difficult to prevent scope creep. We naturally want to be able to help everyone and veered off mission too frequently to help stray animals or animals owned by animal welfare organizations. Those are both fine goals, but we learned we are most effective and efficient when we focus our resources solely on our stated mission.’
Information and permissions provided by:
Amy Crum, DVM, President and Founder,
Principle 7: Community engagement can only be sustained by identifying and mobilizing community assets and strengths and by developing the community’s capacity and resources to make decisions and take action.
The One Health Clinic is a broad collaboration of many groups, from academic training programs to local care providers; at the core is an Advisory Board with lived experience of homelessness and community advocacy.
The One Health Clinic (OHC)
Seattle WA (and other sites)
Mission
To provide healthcare to vulnerable individuals and their pets as a family unit through an interdisciplinary approach that includes zoonotic disease, behavioral health, nutrition, and other key areas.
Scope of services
The OHC is a collaboration of many organizations: faculty and staff at the University of Washington and Washington State University; Neighborcare Health, a federally qualified human healthcare provider; and many community partners providing hosting locations, on-site support, and resources. Clients are referred and recruited through community partnerships.
The program started as a means of addressing the preventive and basic healthcare needs of families experiencing homelessness, including healthcare needs of pets. Veterinary care partners and healthcare navigators from a student-led, volunteer street medicine program offered through the University of Washington joined an existing Neighborcare Health Clinic located in an enhanced emergency shelter located in Seattle.
This clinical model of care integrates veterinary and human healthcare, and each visit has both owners and pets checking in with their respective healthcare providers. In the first year that veterinary care was offered, the human healthcare patient load increased by 32%, reflecting that caretakers will often privilege the health and well-being of pets over themselves and access healthcare for themselves when offered in tandem with veterinary care. At the OHC, in addition to clinical care, pet caretakers gain access to other healthcare and services in the community, including resources for pet-friendly housing support and case management.
Both human health science students and veterinary students are trained through this program. The curriculum requires robust preparatory training, including modules on Trauma-informed Care and clinical communication in addition to clinical skills. Instructors conclude each event with One Health-focused, interprofessional rounds to debrief with students on cases as well as discuss common social determinants of health and the importance of maintaining family units.
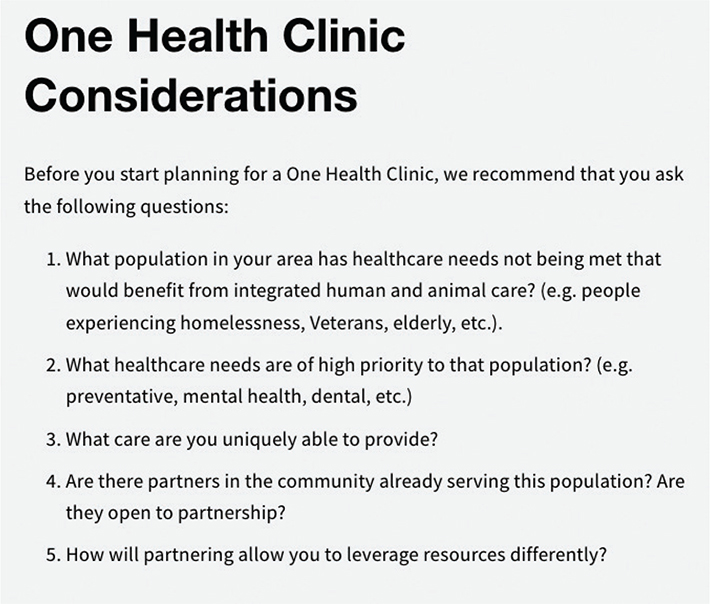
https://www.onehealthclinic.org/toolkit

OHC: The One Health Clinic Interprofessional Team delivering care at New Horizons Youth Shelter in Seattle, WA
The OHC Advisory Board includes individuals with lived experience of being homeless in this community and provides both guidance and connection on how programming is conducted. The creation of a toolkit in 2020 supports other groups across the United States in replicating the OHC integrated care approach.
Mistakes or challenges
A challenge continues to be acting within the scope of services they can provide when the needs extend beyond their scope. Networking with partners to provide additional services – spay/neuter, transportation, more advanced care – makes some of this possible without over-extending the program.
Words of advice
‘Network with as many orgs as you can and make sure you pull together collaborative resources. Do not just drop in and assume a void. We see a lot of redundant services that are not as effective as collaborative projects. Know what else is happening in the area. Listen to your community and be sure that you have their input on what they need and how best to deliver it.’
Information and permissions provided by: Vickie Ramirez, One Health Clinic Coordinator, University of Washington, Katie Kuehl, DVM, One Health Clinic Veterinary Health Director, Washington State University, onehealthclincseattle@gmail.com, Join the toolkit community at www.onehealthclinic.org
Principle 8: Community collaboration requires long-term commitment to have the best chance at a measurable and sustainable impact.
Extensive longitudinal work by RAVS program leads and partners has developed deep collaboration and ethical training alongside high-quality care delivery. The significant investment by all parties is acknowledged and celebrated.
Rural Area Veterinary Services (RAVS), Humane Society of the United States (HSUS)
Mobile, with focus on Native Nations lands in the Western USA
Mission
To preserve and improve the health and welfare of animals, families, and communities by building professional capacity and expanding access to veterinary care in rural communities impacted by poverty and geographic isolation rooted in systemic inequities.
Scope of services
RAVS provides veterinary care in under-served rural communities where families face an array of complex, interconnected barriers to accessing pet care resources. Since its inception over 20 years ago, the dual mission of direct care and teaching/mentorship has responded to the need for veterinary services in rural communities and also the need for practical clinical experience for veterinary students.
The program has grown and evolved significantly over the past 20+ years during which RAVS field teams have provided direct care services in 42 Native Nations communities, 35 non-native rural communities, and 18 countries around the world. While doing this, RAVS has provided hands-on clinical experience and exposure to access to care issues for more than 9,000 veterinary students and professionals.
RAVS utilizes three interconnected approaches: 1. direct care field clinics to preserve and improve animal and community health; 2. clinical training and professional engagement to increase awareness and empower veterinary professionals with skills and experience; and 3. community support to build local capacity for community-based animal care resources. The core field teaching clinics provide MASH medical and surgical veterinary care for dogs and cats at no cost to clients on a first come, first served basis. Clinics are volunteer centered with a small staff team; veterinary and veterinary technician students make up about half of the volunteers.
RAVS teams provide services at the request and invitation of the community. Each clinic is a collaborative event coordinated with local partners. The host community provides a facility to work and camp in, meals for volunteers during the clinic, advertising to the community, and general logistical support during the clinics. Host partners determine eligibility requirements for services (e.g. in some communities, hosts elect to restrict services to local residents or tribal members) and other factors to meet local needs.
Most partnerships are long-standing. Many families have been bringing pets to clinics year after year and know to expect them. Services are advertised to community members/potential clients via flyers, radio, local advocate groups and local social media.
RAVS training consists of a deliberately designed curriculum beginning with pre-clinic learning and evaluation including an extensive online volunteer training manual. Volunteers are required to pass an online training assessment relevant to their area of work. Each day, volunteers are assigned to work in a specific area of the clinic and onsite orientations are provided for anesthesia/recovery, surgery, and medicine/intake/discharge. Printed copies of protocols and reference guides are available throughout the clinic to ensure consistency of protocols and care. A staff lead in each area coordinates work, oversees patient care, and supports training/mentorship. Staff members in each area mentor and supervise professional volunteers (veterinarians, veterinary technicians, and assistants) who are in turn working closely with students. Students are closely supervised and supported by experienced anesthesia technicians. In surgery, students work one-on-one with a veterinarian in all procedures. Guidelines exist for cases that may be complex or have increased risk.
At the end of each day, rounds review cases of the day and relevant clinical and/or professional topics. Rounds have been especially helpful for discussions on access to care and systemic inequities. Working directly within a community where people face significant barriers to accessing basic services increases awareness of the impacts of systemic inequity and of the power veterinary professionals have to effect change. Knowledge, approaches, and philosophies experienced in these clinics can be incorporated into daily practice anywhere – offering a broader spectrum of care and more fully leveraging skill sets to enable any veterinary professional to expand access to care in their own community.
Because of longstanding relationships with partners, RAVS is often contacted for assistance when animal needs or opportunities arise outside of field clinics. The program expanded to include Community Animal Care projects which support locally led community initiatives with funding, consultation, and general support to build capacity and strengthen relationships to facilitate community-led access to care solutions. Several community-based animal care efforts have developed within partner communities.
Mistakes or challenges
MASH teaching clinics incorporating large numbers of volunteers are logistically complicated. They are time and staff-intensive and require skill sets beyond clinical competency. The program must balance the sometimes competing priorities of teaching/mentorship, patient care, and overall impact. While the program utilized far fewer staff in the earlier years, overall human and animal experience has improved by having a more consistent experienced team in the field, which reduces stress and improves job satisfaction.
Another challenge has been need/demand far exceeding capacity on a daily and an annual basis. In the early years, clinics were scheduled based entirely on the number of requests without first clearly defining clinic capacity. The strain on personnel was significant and volunteers did not always have the support needed to thrive. Annual clinic planning is now approached more strategically with commitments made based on actual capacity (funding, staffing, and other resources). This approach has proven to be far more sustainable and rewarding.
Finally, the program has evolved techniques to increase clinic efficiency to reduce working hours per day while maintaining caseload. Extremely long work hours in years past contributed to staff burnout and decreased volunteer satisfaction, overall team performance, and patient care. Field work is physically and emotionally taxing. Continual process evaluation and adjustment have helped to balance the various demands of caseload, teaching, and team health.
Words of advice
‘Consistent communication, following through on our commitments and being adaptable to accommodate challenges are essential for all areas of our work. Key approaches include asking about community priorities and resources, revisiting these conversations on a regular basis, and making every effort to accommodate requests and needs while being honest about our capacity. With large teams heavily comprised of volunteers from a range of professional backgrounds, we find it helpful to incorporate discussions about cultural humility and an empathic, family centered approach. We share our philosophy that people who bring their pets to us have unique expertise in knowing what is best for their families and we work together to find the most appropriate course of action. These discussions and situations can sometimes be challenging, but we hold one another accountable to presume good intent and meet clients and their pets without judgment.’
Information and permissions provided by
Windi Wojdak, RVT – Senior Director, RAVS
Principle 9: Successful community collaboration requires continual reflection, both individually and as a group. Accountability and assessment of VCE programming is crucial for continued success.
The ASPCA Spay Neuter Alliance has engaged in consistent measures and assessments in adapting and refining programming over the last two decades, including expanding into mentorship for the replication of services in other communities.
ASPCA Spay Neuter Alliance (ASNA)
Asheville, NC
https://www.aspca.org/helping-people-pets
https://www.aspcapro.org/training/aspcar-spayneuter-alliance-training
Mission
The ASPCA’s mission is to provide effective means for the prevention of cruelty to animals throughout the United States. Originally founded in 1994 and a program of the ASPCA since 2015, ASNA focuses on the use of high quality, high volume spay-neuter (HQHVSN) surgery to reduce unwanted cat and dog populations and prevent unnecessary euthanasia.
Scope of Services
ASNA has provided over 500,000 spay-neuter surgeries in Western North Carolina. In addition to their direct care mission for companion animals, ASNA has training programs for veterinarians, technicians, support staff, and fourth-year veterinary students. Their campus in Asheville North Carolina hosts hundreds of veterinary professionals and students per year for closely supervised, intensive training in a purpose-built surgical training center. Participants gain the techniques and expertise to apply their new skills confidently and successfully in their communities. ASNA also offers clinical mentorships which provide on-site and remote coaching for entire clinic teams so they can better work together in providing HQHVSN services. This mentorship program has created a network of professionals committed to making a difference for people and animals in their communities.
Re-evaluation and assessment are key to ASNA’s mission and success. When it became apparent that their local reach needed to expand, ASNA started a daily transport program to increase access to services across the region. When it came time to take the model on the road, the training program extended the reach of ASNA’s expertise across the United States and internationally. ASNA’s work has led to the development and advancement of HQHVSN practice, as well as the publication of The Association of Shelter Veterinarians’ 2016 Veterinary Medical Care Guidelines for Spay-Neuter Programs, nationally recognized as HQHVSN guidelines. Interactive educational approaches and a commitment to meeting each learner where they are have resulted in a robust educational experience for individuals and teams and changed the landscape of accessible spay/neuter services for families and communities. Consistent collection of feedback and ongoing self-assessment has contributed to the development of expertise and replication of successful programming.

ASNA: ASNA’s HQHVSN programming and training has evolved over decades in response to consistent and comprehensive assessment and evaluation.
Mistakes or challenges
In the beginning, the ASNA team believed that everyone would see the benefit of their work and be in support. However, some professionals – particularly veterinarians in private practice – did not understand the work nor see the welfare implications of animal overpopulation through the same lens. ASNA worked diligently to gain credibility by inviting detractors to the table, as well as standardizing protocols and techniques with the help of veterinary experts.
Words of advice
‘Persevere if you know the mission is worthy. We could have given up in the early years but when I think of all the animals & people we’ve helped and all the lives spared, I know that staying the course was the only path.’
Information and permissions provided by:
Karla Brestle, DVM, Senior Director, Training Programs, ASPCA Spay/Neuter Alliance