ORIGINAL RESEARCH ARTICLE
Barriers and Lack of Access to Veterinary Care in Canada 2022
Linda S. Jacobson1, Kyrsten J. Janke1, Kevin Probyn-Smith2 and Kate Stiefelmeyer2
1Toronto Humane Society, Toronto, ON, Canada; 2Kynetec Canada, Guelph, ON, Canada
Abstract
Introduction: Despite concerns about access to veterinary care in Canada, there are no previously published national survey data. The study aimed to estimate the prevalence of barriers to veterinary care faced by Canadian dog and cat owners, and to identify associated factors.
Methods: This was a national online survey conducted in mid-2022, the third year of the COVID-19 pandemic. It was nationally representative of English and French-speaking Canadian adults as regards region, age, and sex.
Results: Eighteen per cent of the respondents (440/2,500) could not access wanted or needed preventative veterinary care in the past 12 months; 12% (305/2,500) could not access sick care; and 8% (195/2,500) could not access emergency care. The most frequent barriers were the inability to afford care (preventative – 124/440, 28% of those who were unable to access care; sick – 75/305, 25%; emergency – 34/195, 17%); and the inability to obtain an appointment (preventative – 95/440, 22% of those who were unable to access care; sick – 80/305, 26%; emergency – 47/195, 24%). Twenty-one per cent (522/2,500) could not access other pet needs, most frequently pet food (43% of those who lacked access); grooming (34%); and training (28%). Recent immigrants (<5 years) and young people (18–34 years old) were more likely to report barriers. Affordability and appointment availability were the two most frequently occurring barriers.
Conclusions: This survey identified a large number of pet owners who faced barriers to veterinary care. There is a need for industry leaders, educators and regulators to help support initiatives to expand access to care.
Keywords: accessible veterinary care; access to care; barriers to care; non-medical pet care; online survey; nationwide; Canada
Citation: Journal of Shelter Medicine and Community Animal Health 2024, 3: 72 - http://dx.doi.org/10.56771/jsmcah.v3.72
Copyright: © 2024 Linda S. Jacobson et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 6 November 2023; Revised: 13 January 2024; Accepted: 17 January 2024; Published: 28 February 2024
Competing interests and funding: The Canadian Animal Health Institute included the access to care questions in the biannual Canadian Pet Ownership Study. Zoetis Canada provided access to the complete Pet Ownership Study report.
Corresponence: Linda S. Jacobson Email: ljacobson@torontohumanesociety.com
Reviewers: Terry Spencer, Jeff Norris
Supplementary material: Supplementary material for this article can be accessed here.
Access to veterinary care (AVC) has received growing attention in recent years.1–9 Pets who are not presented for care remain largely invisible to veterinarians and policymakers, creating a vicious cycle in which this important welfare concern is not adequately recognised and cannot be appropriately addressed. Lack of AVC and other pet resources is likely to be a substantial problem in Canada, as elsewhere
Multiple barriers to AVC exist, including affordability, transport, clinic location and availability, communication, cultural or language barriers, negative previous encounters with veterinarians, lack of trust in veterinarians, and lack of knowledge.2,3,8,10 Barriers have been associated with ethnicity, low income, young age, geographic area, and lower level of education.10,11 A 2017 American Access to Veterinary Care Coalition (AVCC) study estimated that 23% of peta-owning families had been unable to access wanted or needed preventative care for their pets over the past 2 years; 14% had been unable to access sick care; and 8% had been unable to access emergency care.11 A veterinary care map of the 48 contiguous United States (US) states was recently added to the knowledge base and provides a visual representation of the distribution and magnitude of the problem.12,13 Several surveys, primarily focused on the US, have addressed the impacts of the coronavirus disease 2019 (COVID-19) pandemic on veterinary care and the veterinary industry.14–16
A spectrum of care, family-centred approach,4,17–20 has been advocated as a way to broaden AVC. In a 2022 US study, most veterinarians surveyed said the pandemic had changed their views on veterinary medicine and vulnerable populations, and that they would want to play a greater role in supporting vulnerable clients.14 This is likely also to be the case in Canada.
In 2022/23, disposable income for the bottom 20% of Canadian households was $6,41521 and the official poverty rate was 7.4%.22 The cost of veterinary care in Canada from 2007–2020 has markedly outpaced inflation.23 The COVID-19 pandemic resulted in product shortages and delays in delivery,16 which led to higher costs for pet food, alongside increased requests from pet food banks and decreased donations.24 Despite some important insights and studies,1,3,8,25 there are no comprehensive data about lack of AVC and other basic needs for companion animals in Canada.
The objectives of the current study were to estimate the prevalence of barriers to veterinary care faced by pet owners in Canada, and identify associated demographic and geographic factors. A secondary objective was to identify and report other important pet care needs that could not be accessed.
This initial survey provides baseline data to help inform decision-making for regulators, educators, animal welfare agencies, professional associations, companion animal practices, and corporate groups in Canada. The survey also provides a unique snapshot of AVC in Canada during the COVID-19 pandemic, allowing for later comparisons.
Materials and methods
The survey was conducted in June and July 2022, as an addition to the Canadian Pet Ownership Study.26 For the purposes of this study, ‘pets’ are defined as dogs and cats. The study is commissioned by an industry association, the Canadian Animal Health Institute (CAHI), and is carried out by Kynetec. The CAHI members, who fund the study, kindly permitted the shelter investigators to add several AVC questions (Table 1). The AVC responses were provided to us as counts, not as individual responses, while data from the larger study were available in summary form.26
| The next set of questions we are going to ask you about are about access to veterinary care in the past 12 months. You will be asked about PREVENTATIVE care, SICK care and EMERGENCY care for your pet(s) separately. |
| The first type of care is PREVENTATIVE care. These are services a pet receives to avoid illnesses, diseases, and behavioral problems. This includes such things as annual exams; shots or vaccinations; heartworm, flea, or tick prevention; and advice about how to care for your pet. |
1A. In the past 12 months, has there been a time that you wanted or needed PREVENTATIVE care for your pet(s), but were not able to get it? Options: Yes/No |
1B. You mentioned you were not able to get PREVENTATIVE CARE for your pet(s) in the past 12 months. What was the reason you were not able to get care for your pet(s)? Please select all that apply. Options (order randomized): |
|
| Options in bold type were in addition to those provided in the AVCC survey11 upon which these questions were based. |
1C. Which of those reasons would you consider to be the biggest reason for not being able to get the PREVENTATIVE care you wanted or needed? Select one. Options as for 1B. |
| The second type of care is SICK care. This type of care includes treatment for an illness, physical injury, or behavioral problem that is NOT an emergency requiring immediate care. |
| 2A-C. Same questions and options as for 1A-C but for SICK care. |
| The third type of care is EMERGENCY care. This type of care includes treatment for an illness, physical injury, or behavioral problem that needed immediate treatment. |
| 3A-C. Same questions and options as for 1A-C but for EMERGENCY care. |
4. Is there anything other than veterinary care that is important for your pet, that you are not able to access currently? Select all that apply. |
|
The CAHI commissioned the study in 2004, 2007, and biennially since 2010. The 2022 study was conducted using methodology in use since 2016, which includes a nationally representative telephone survey of Canadian adults (pet owners and non-owners) and a nationally representative online survey of pet owners. A telephone survey is used to establish the frequency of pet ownership, and an online survey is used for all other questions. Both surveys were fielded in English and French. Each respondent represented one household.
An existing Canadian consumer panel was surveyed. The online survey of pet owners consisted of 2,500 completed surveys, with an average length of 22 min. It was a nationally representative sample of English and French-speaking Canadian pet owners as regards region, age, and sex. The response rate was 69%, and the sample size resulted in a margin of error of 2% at a 95% confidence interval (CI).
The CAHI survey includes questions about citizenship, age, sex, household income, and location (Supplementary file 1). Additional questions about ethnicity and size and type of location were added for the AVC study (Supplementary file 1), as we hypothesised that these factors would impact AVC. Demographic and geographic variables were assessed to determine associations with barriers to care.
The AVC questions (Table 1) were modelled, with permission, on a section of the CARE Pet Owners Survey Instrument used for the 2017 US AVCC study.11 Respondents were asked about all barriers to veterinary care that they faced (‘select all that apply’). If more than one was selected, they were asked to select the primary, or most important, barrier (‘which of those reasons would you consider to be the biggest reason for not being able to get the care you wanted or needed?’). Barriers were listed in randomised sequence. The data analysis focused on primary barriers, in alignment with the AVCC analysis. We used the AVCC questions relating to inability to get wanted or needed care, but did not include AVCC follow-up questions about what specific care was wanted or needed (e.g. vaccination), or how many times the owner had been unable to access the care. We included the barriers to care listed in the AVCC study, and added the inability to get an appointment or to find a veterinarian taking new patients (Table 1). We also added a question about access to other types of pet care (Table 1). Demographic categories were structured differently from the AVCC study, and used existing methodology for the CAHI survey. Again following existing methodology, our study asked about barriers in the past year, compared with 2 years for the AVCC study.
Data analysis
The data were analyzed using Microsoft Excel with XLSTAT v19.1 plugin. Chi-square tests were used to calculate the probability of a demographic or geographic variable being significantly associated with the inability to access care. If the Chi-square was significant, a post-hoc Fisher exact test was used to determine which groups significantly differed. Because of small cell counts, the Fisher exact test was used to calculate the probability that a demographic or geographic variable was significantly associated with a specific primary barrier to care. The alpha level to determine statistical significance was adjusted for multiple tests using the Bonferroni correction. There were six independent variables, resulting in a significance threshold of ≤ 0.008 (0.05/6).
Results
Access to veterinary care
When asked if they had been able to access wanted or needed veterinary care in the past 12 months, 18% of respondents (440/2,500; 95% CI 16–20%) reported that they had been unable to access preventative care; 12% had been unable to access sick care (305/2,500; 95% CI 10–14%); and 8% had been unable to access emergency care (195/2,500; 95% CI 6–10%).
Barriers to different types of veterinary care
Figure 1A shows primary barriers, i.e. ‘which of those reasons would you consider to be the biggest reason for not being able to get the care you wanted or needed?’. For those who were unable to access care, the most frequent barriers were the inability to afford care (preventative care 124/440, 28%; sick care 75/305, 25%; emergency care 34/195, 17%) and being unable to obtain an appointment (preventative care 95/440, 22%; sick care 80/305, 26%; emergency care 47/195, 24%). Alternative primary barriers were reported by 3–12% of respondents (Figure 1A). ‘Other’ was selected by 15% for preventative care; 8% for sick care; and 9% for emergency care. Figure 1B shows results for all barriers (‘select all that apply’), and reflects similar patterns.
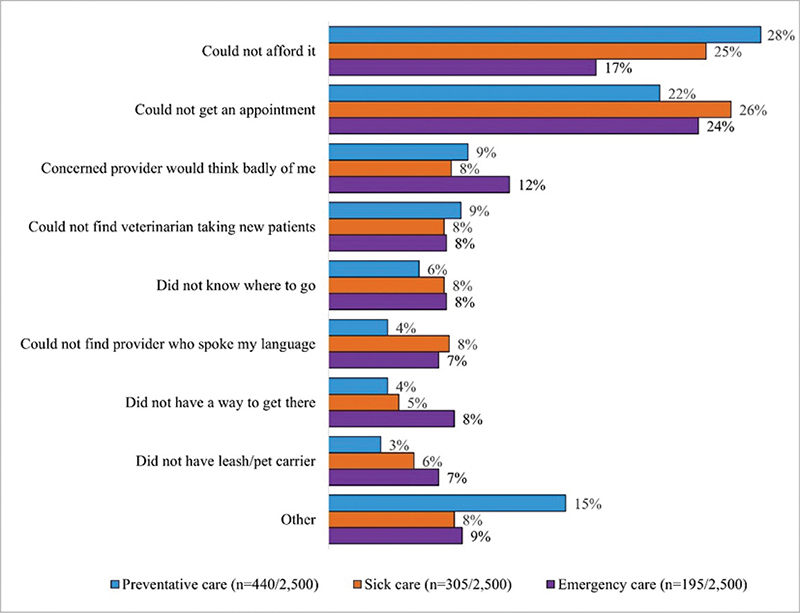
Fig. 1A. Barriers reported by respondents who were unable to access veterinary care, Canada 2022. Note that percentages are percentage of respondents who could not access care, not percentage of total respondents. Primary barriers (‘which of those reasons would you consider to be the biggest reason?’).
Fig. 1B. Barriers reported by respondents who were unable to access veterinary care, Canada 2022. Note that percentages are percentage of respondents who could not access care, not percentage of total respondents. All barriers (‘select all that apply’).
Associations between inability to access veterinary care and demographic or geographic variables
This portion of the analysis assessed whether the inability to access care was associated with demographic or geographic variables, irrespective of the reason that the care could not be accessed. Some groups could not be statistically analyzed because of sparse data cells. These were: ethnic groups the two types of Indigenous communities included in the location variable (Supplementary file 1); and most ‘other/don’t know/prefer not to answer’ groups.
Citizenship was significantly associated with barriers to AVC (Figure 2A–C; Supplementary file 2). Compared with other citizenship groups, respondents who had been in Canada for less than 5 years were significantly more likely, and Canadian-born respondents significantly less likely, to report barriers to all three types of care. Young adults (18–34) were significantly more likely, and older adults (65+) significantly less likely, to report barriers to all three types of care.
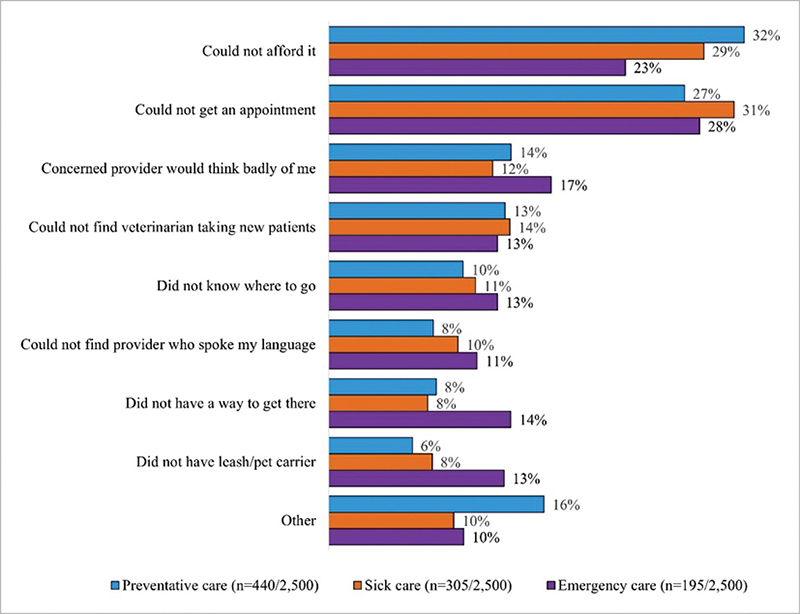
Fig. 2A. Demographic and geographic factors associated with barriers to access to preventative veterinary care, Canada 2022 (440/2,500 respondents; 18%). Statistically significant differences within groupings are shown using dark blue solid (significantly more likely to report barriers) and diagonal shading (significantly less likely to report barriers). Note that percentages shown are percentage of respondents within a subgroup e.g. age 18-34) who could not access care, not percentage of total respondents.
Fig. 2B. Demographic and geographic factors associated with barriers to access to sick veterinary care, Canada 2022 (305/2,500 respondents; 12%). Statistically significant differences within groupings are shown using dark blue solid (significantly more likely to report barriers) and diagonal shading (significantly less likely to report barriers). Note that percentages shown are percentage of respondents within a subgroup e.g. age 18-34) who could not access care, not percentage of total respondents.
Fig. 2C. Demographic and geographic factors associated with barriers to access to emergency veterinary care, Canada 2022 (195/2,500; 8%). Statistically significant differences within groupings are shown using dark blue solid (significantly more likely to report barriers) and diagonal shading (significantly less likely to report barriers). Note that percentages shown are percentage of respondents within a subgroup e.g. age 18-34) who could not access care, not percentage of total respondents.
There were no significant differences by sex, income grouping or region of Canada for the inability to access veterinary care (Figure 2A–C). Respondents living in large cities (population ≥ 1 million) were more likely to report barriers to emergency care, while those living in medium-sized cities (population 100,000–999,999) were less likely to report barriers to this type of care (Figure 2C).
For all related comparisons and P values, see Supplementary file 2.
Associations between the primary barrier to veterinary care and demographic or geographic variables
This portion of the analysis assessed relationships between the primary reason for being unable to access a particular type of veterinary care, and demographic and geographic variables. Significant associations are shown in Table 2.
Males were significantly less likely (P = 0.003), and females significantly more likely (P = 0.003), to report cost as a barrier to accessing preventative care (Table 2). Respondents with annual household income <$50,000 were significantly more likely than those with larger household incomes to report an inability to afford care as the primary barrier to access to all three types of care (P < 0.001, P = 0.005, P = 0.006 for preventative, sick and emergency care, respectively). Those with household income of $100,000–$199,000 were significantly less likely (P = 0.004) to report being unable to afford care as the primary barrier to sick care, and significantly more likely (P = 0.008) to report the inability to obtain an appointment as the primary barrier to this type of care. Being unable to afford preventative and sick care was significantly more frequent in the West (P < 0.001, P = 0.001) compared with other regions of Canada, while being unable to obtain an appointment for preventative care was significantly less frequent (P = 0.007). Residents of medium-sized cities were significantly more likely to report being unable to obtain an appointment as their primary barrier to sick care, compared with other location types (P = 0.002). Respondents from Quebec reported the inability to afford preventative care significantly less frequently than other regions (P = 0.001).
All significant findings for this analysis are detailed in Table 2. For all related comparisons and P values, see Supplementary files 3–5.
Lack of access to other types of pet care
Twenty-one per cent of respondents (522/2,500) reported being currently unable to access non-veterinary pet needs. These were pet food (43% of those unable to access non-veterinary needs); grooming (34%); training (28%); pet medication (23%); pet sitting or boarding (16%); and ‘Other’ (8%). Groups that were significantly more likely to report barriers to non-veterinary pet care were immigrants (<5–19 years), young adults, those in the lowest income group and those in large cities (Figure 2D). Groups significantly less likely to report these barriers were Canadian-born respondents, older age groups (55–65+) and those in medium-sized cities.
Fig. 2D. Demographic and geographic factors associated with barriers to non-veterinary pet care, Canada 2022 (522/2,500; 21%). Statistically significant differences within groupings are shown using dark blue solid (significantly more likely to report barriers) and diagonal shading (significantly less likely to report barriers). Note that percentages shown are percentage of respondents within a subgroup e.g. age 18-34) who could not access care, not percentage of total respondents.
Discussion
The 2021 Census reported 14.98 million households in Canada.27 An estimated 60% of households owned at least one dog or cat in 2022.26 Extrapolating the study findings to all pet-owning households, this would amount to an estimated 1.62 million households facing barriers to preventative care; 1.08 million to sick care; and 719,000 to emergency care. Each household represents one or more pets that could not receive wanted or needed care. The 2022 CAHI survey reported that 27% of pets had not visited a veterinary clinic in the past 12 months (‘non-medicalized’).26 The survey question focuses on the number of pets that saw a veterinarian (‘medicalized’) and historically has not asked why the remainder did not. It has not previously been possible to estimate how many pets needed veterinary care but did not receive it, as opposed to those that did not need care or where the guardian did not perceive a need. While our data do not allow direct calculations, they do suggest that a substantial proportion of the non-medicalized pets needed care but did not receive it.
Care must be taken when interpreting the study findings. There were a number of apparent contradictions between the statistical analyses for overall barriers to care (i.e. was a barrier present, yes/no) (Figure 2A–C) and those for specific barriers (i.e. when a barrier was present, which one was the most important) (Table 2). This is most likely because of an averaging effect for overall barriers. For example, if the primary barrier for a low-income group was cost, and the primary barrier for a high-income group was finding an appointment, the overall lack of access to care would be similar, while a difference would be detected for the specific barriers faced – as was indeed the case. The findings are consistent with this interpretation.
The inability to afford care and obtain an appointment were the most important barriers to care. Although only 14% of respondents in an Ontario survey had not visited a veterinarian in the past year, cost as a primary barrier was proportionately similar to our study, with 36% of those that had not accessed care (5% of total respondents) not having done so because the care was too expensive.28 Almost a quarter of those respondents said they were willing to pay <$500 for a medical emergency involving their pets and more than half felt that pet food was too expensive. The inability to obtain appointments might be pandemic-related, but this problem may in fact have preceded the pandemic. The pandemic resulted in substantial changes to the provision of veterinary services, with decreased availability of preventative care, slower appointments, and subsequent backlogs.14,15,24 Despite this, a similar percentage of pets visited Canadian veterinarians in the 12 months preceding mid-2022, compared with 2020 and 2018.26 There were also similar numbers of visits per pet.26 Most veterinary practices in Canada reported unchanged or higher revenues, and served more clients, in 2020 and 2021.16,29 Telemedicine was widely used early in the pandemic16,30 and may have expanded AVC.14 However, in 2019, prior to the pandemic, approximately half of veterinary clinics reported that > 80% of appointments were booked, and almost one in five regularly turned away clients.31 The Canadian Veterinary Medical Association has identified a veterinary capacity shortage as a critical challenge for the profession.31,32
More respondents reported barriers to preventative care than sick and emergency care, which are more time-sensitive and can cost substantially more. One explanation might be that sick and emergency care were prioritised over preventative care during the pandemic, but this would not account for similar findings in the pre-pandemic AVCC study.11 The most plausible explanation is that these types of care are required less frequently than preventative care. Routine examinations were the most frequent reason for veterinary visits in 2022 (83% of dog visits, 75% of cat visits).26
Recent immigrants and youth faced barriers to all types of pet care assessed. Canada’s labour market and, increasingly, population growth are dependent on immigration – 23% of census respondents in 2021 were immigrants.33 Although our study was unable to analyse results for ethnic and racial minorities, immigrant status is a partial proxy for racialization – 70% of racialized people in Canada were not Canadian-born, and 62% of recent immigrants are from Asia and the Middle East.33,34 The study findings therefore suggest that racialized minority groups might face greater barriers to AVC in Canada. The study was not able to analyse results for Indigenous respondents, but Indigenous communities are known to face substantial barriers to veterinary care, including financial, cultural and geographic barriers.35
Females reported greater cost barriers than males, consistent with the fact that Canadian women continue to earn less than men.36 Few regional differences were found in our study, possibly because the results grouped Canada into four large regions, each of which is socioeconomically and geographically diverse. Canada is one of the most decentralised countries among the Western democracies, with large regional variations in unemployment and poverty rates.37,38 The regional results are therefore difficult to interpret, and this aspect requires further investigation.
Approximately one in five respondents in our study reported barriers to non-veterinary types of care. There was a similar pattern to veterinary care regarding which groups were most impacted. Pet food insecurity, in particular, is an important source of distress for pet guardians and an important contributing factor to relinquishment.39,40 Our data support the need for funding and assisting pet food banks in Canada.41 The provision of additional products and services alongside veterinary care in under-served communities is likely to have substantial health and welfare benefits.
The percentage of Canadian respondents who were unable to access preventative veterinary care was slightly lower than the nationally representative 2017 US AVCC study (18% [CI 16–20%] vs. 23% [CI 22–24%]),11 with similar prevalence for sick care (12% vs. 14%) and emergency care (8% vs. 8%). Cost was a more dominant barrier in recent US studies (~50–80%).10,11 than in our study, and a recent Ontario survey.28 This is unlikely to be because of differences in the nature of veterinary care between the US and Canada. These countries provide similar veterinary medical education and utilise the same national licensure examinations.42,43 The cost of care has escalated in both countries in recent years.5,23 One reason for the difference might be lower income inequality and more post-tax income transfers to lower-income families in Canada.38,44 Canada also provided strong income support during the pandemic, resulting in increased disposable income.38 Some of the difference could relate to wording of the questions. The US studies did not ask about availability of appointments, and a greater proportion of our respondents would have had to select different responses without this option. Difficulty obtaining appointments might also have prevented cost (or other) considerations from becoming the salient factor for some respondents.
Barriers to veterinary care do not exist in isolation, but in the context of the same social determinants of health that impact human health provision,2,6,45 and the political and policy frameworks within which these exist. An effective safety net is needed for pets marginal to the existing care provision model.46 Currently, no federal programmes exist in Canada to help improve access to care for pets.8 Animal shelters, rescues and outreach groups can provide some care, typically to the most marginalised, but are hampered by chronic resource limitations, lack of a cohesive strategy, and regulatory restrictions. Canadian figures are not available, but shelter and community clinics provided less than 5% of veterinary care in the US in 2017.11 The Canadian animal sheltering sector is small compared with the broader veterinary industry.47,48 Participation from the veterinary community as a whole is needed, but individual shelters and private practices, already struggling with capacity shortages, staff stress and burnout, should not be expected to tackle this problem unsupported.
Limitations
There were many advantages to adding questions to an established survey, and this was a fruitful collaboration that made it possible to generate these important baseline data. Advantages of this approach included feasibility, costs, timing, and access to established methodology and expertise. However, there were also a number of drawbacks, including a limited number of AVC questions and lack of access to individual responses. As a result of the latter, it was not possible to utilise multiple regression analysis to account for confounding effects of different variables.
The survey targeted English and French speakers, and was not designed to be representative of different ethnic groups. For this reason, it may not be representative of the population beyond the targeted demographics of region, age and sex. The study was not able to provide insights into the needs of those most likely to face barriers to pet care, such as remote Indigenous communities or those dealing with disability, homelessness, mental illness or unemployment. Such insights are important for targeted solutions and should be addressed by future studies.
Geographic factors were almost certainly underestimated in this study because only large regions were assessed. Clinic catchment areas and the ratio of care providers to population vary widely in the US,7 and resources are skewed towards more affluent areas of cities.49 The paucity of veterinary and other services in remote Indigenous communities, in particular, is well-recognised.8,25
The ‘Other’ barrier category appeared important and had one significant association (Supplementary file 4), but was not interpretable. Future versions of this survey should endeavour to ascertain what these additional barriers are.
Unlike other studies that focused on the initial year of the pandemic,14–16 ours took place in its third year. Pandemic measures progressively eased during the period under consideration.50 As this is the first survey of its kind in Canada, it was not possible to directly assess the impact of the COVID-19 pandemic on AVC. The authors hope to repeat the AVC questions as part of the biennial CAHI survey, to allow assessment of trends and comparison of the pandemic and post-pandemic periods.
Conclusions
This survey identified a large number of pet owners who faced barriers to veterinary care. Immigration status and age were the two dominant demographic factors that affected access to care, while cost and appointment availability were two most frequently occurring barriers to care. The study found that these factors and barriers were at play across the spectrum of pet health, including preventative, sick, emergency, and non-veterinary care.
Broadening AVC will require sustainable funding models, education, guidance on spectrum of care approaches, assistance from large corporate groups, expanded care provision capacity, and flexible and progressive regulatory frameworks. A wider range of care provision types is needed, with more clinics that utilize accessible models.
Acknowledgements
With grateful thanks to: Catherine Filejski and Emily Bond (CAHI), Gavin Baines and Stevan Agbaba (Zoetis), Gina Lockwood (independent statistical consultant), Linda Daugherty (University of Tennessee), Kate Atema (PetSmart Charities), Barbara Cartwright, Kathy Duncan and Toolika Rastogi (Humane Canada), Phil Nichols and Karen Ward (Toronto Humane Society). We thank the Board, management and staff of Toronto Humane Society for their support.
Author notes
An abbreviated summary of key study findings was included in the 2022 Pets in Canada report.
References
| 1. | Harding MJ. Access to veterinary care for low-income Canadians. Can Vet J. 2018;59(10):1121–1122. |
| 2. | Lavallee E, Mueller MK, McCobb E. A systematic review of the literature addressing veterinary care for underserved communities. J Appl Anim Welf Sci. 2017;20:1–14. doi: 10.1080/10888705.2017.1337515 |
| 3. | Lem M. Barriers to accessible veterinary care. Can Vet J. 2019;60:891–893. |
| 4. | Stull JW, Shelby JA, Bonnett BN, et al. Barriers and next steps to providing a spectrum of effective health care to companion animals. J Am Vet Med Assoc. 2018;253(11):1386–1389. doi: 10.2460/javma.253.11.1386 |
| 5. | Einav L, Finkelstein A, Gupta A. Is American pet health care (also) uniquely inefficient? Am Econ Rev. 2017;107(5):491–495. doi: 10.1257/aer.p20171087 |
| 6. | Neal SM. Correlating access to primary medical care and veterinary care providers: a novel application of spatial gravity modelling. Vet Sci. 2023;10(9):1–11. doi: 10.3390/vetsci10090565 |
| 7. | Neal SM, Greenberg M. Veterinary care deserts: what is the capacity and where is it? J Shelter Med Community Anim Health. 2022;1(1):1–8. doi: 10.56771/jsmcah.v1.2 |
| 8. | Roberts C, Woodsworth J, Carlson K, Reeves T, Epp T. Defining the term “underserved:” a scoping review towards a standardized description of inadequate access to veterinary services. Can Vet J. 2023;64(10):941–950. |
| 9. | Blackwell MJ, O’Reilly A. Access to veterinary care–a national family crisis and case for one health. Adv Small Anim Care. 2023;4(1):145–157. doi: 10.1016/j.yasa.2023.05.003 |
| 10. | Park RM, Gruen ME, Royal K. Association between dog owner demographics and decision to seek veterinary care. Vet Sci. 2021;8(1):1–19. doi: 10.3390/VETSCI8010007 |
| 11. | Wiltzius A, Blackwell M, SB K, et al. Access to Veterinary Care: Barriers, Current Practices, and Public Policy. 2018. https://avcc.utk.edu/avcc-report.pdf. Accessed September 26, 2019. |
| 12. | Neal SM, Greenberg MJ. Putting access to veterinary care on the map: a veterinary care accessibility index. Front Vet Sci. 2022;9:1–8. doi: 10.3389/fvets.2022.85764413 |
| 13. | Veterinary Care Accessibility Project. The Veterinary Care Accessibility Score. 2022. https://www.accesstovetcare.org/vcas-map. Accessed August 3, 2023. |
| 14. | Smith SM, George Z, Duncan CG, Frey DM. Opportunities for expanding access to veterinary care: lessons from COVID-19. Front Vet Sci. 2022;9:1–20. doi: 10.3389/fvets.2022.804794 |
| 15. | Owczarczak-Garstecka SC, Furtado T, Graham TM, et al. Impacts of COVID-19 on owner’s veterinary healthcare seeking behavior for dogs with chronic conditions: an exploratory mixed-methods study with a convenience sample. Front Vet Sci. 2022;9:1–20. doi: 10.3389/FVETS.2022.902219 |
| 16. | CM Research. COVID-19: Global Pandemic Impact on the Veterinary Market. 2021. https://www.canadianveterinarians.net/media/bftkzksf/vet-survey-2020-part-1-covid-19-global-pandemic-impact-on-the-veterinary-market.pdf. Accessed July 3, 2023. |
| 17. | Evason M, Stein M, Stull J. Impact of a spectrum of care elective course on third-year veterinary students’ self-reported knowledge, attitudes, and competencies. J Vet Med Educ. 2022;50:590–598. doi: 10.3138/jvme-2022-0010 |
| 18. | College of Veterinarians of Ontario. Position Statement: Balancing Available Health Care Options and Client Access to Veterinary Care. 2022:1–3. https://www.cvo.org/standards/balancing-available-health-care-options-and-client-access-to-veterinary-care. Accessed August 30, 2023. |
| 19. | Brown CR, Edwards S, Kenney E, et al. Family quality of life: pet owners and veterinarians working together to reach the best outcomes. J Am Vet Med Assoc. 2023;261(8):1238–1243. doi: 10.2460/javma.23.01.0016 |
| 20. | Englar RE. Recasting the gold standard – part I of II: delineating healthcare options across a continuum of care. J Feline Med Surg. 2023;25(12):1–11. doi: 10.1177/1098612X231209855 |
| 21. | Statistics Canada. Distributions of Household Economic Accounts for Income, Consumption and Saving of Canadian Households, Second Quarter 2022. https://www150.statcan.gc.ca/n1/daily-quotidien/221003/dq221003b-eng.htm. Accessed December 11, 2023. |
| 22. | Statistics Canada 2023. Canadian Income Survey, 2021. 2023. https://www150.statcan.gc.ca/n1/daily-quotidien/230502/dq230502a-eng.htm?indid=11361-1&indgeo=0. Accessed December 11, 2023. |
| 23. | Nichols PJH, Ward KA, Janke KJ, Jacobson LS. Trends in companion animal access to veterinary care in Canada, 2007–2020. Can Vet J. 2024:65(1):49–58 |
| 24. | Muzzatti SL, Grieve KL. Covid cats and pandemic puppies: the altered realm of veterinary care for companion animals during a global pandemic. J Appl Anim Welf Sci. 2022;25(2):153–166. doi: 10.1080/10888705.2022.2038168 |
| 25. | Baker T, Rock M, Bondo K, van der Meer F, Kutz S. 11 Years of regular access to subsidized veterinary services is associated with improved dog health and welfare in remote Northern communities. Prev Vet Med. 2021;196:105471. doi: 10.1016/j.prevetmed.2021.105471 |
| 26. | Canadian Animal Health Institute. Canadian Pet Ownership 2022, August 12, 2022:1–46. |
| 27. | Statistics Canada. Census Profile, 2021 Census of Population. 2021. https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/details/page.cfm?Lang=E&DGUIDList=2021A000011124&GENDERList=1&STATISTICList=1&HEADERList=0&SearchText=Canada. Accessed August 18, 2023. |
| 28. | Ontario Veterinary Medical Association. Ontario Pet Owners Report. 2023. https://www.ovma.org/assets/1/6/2023 Pet Owners Report.pdf. Accessed January 11, 2024. |
| 29. | Doherty. A strong year for Canadian veterinarians: results of the 2021 CVMA Practice Owners Economic Survey. Can Vet J. 2022. https://pubmed.ncbi.nlm.nih.gov/35784771/. Accessed September 28, 2022. |
| 30. | Ontario Veterinary Medical Association. Practice Survey Results. 2020. https://www.ovma.org/assets/1/6/NewsHound_April-20-Final.pdf. Accessed July 18, 2023. |
| 31. | Canadian Veterinary Medical Association. CVMA Workforce Study Final Report. May 2020:1–79. https://www.canadianveterinarians.net/media/ak3lonad/2020-cvma-workforce-study-final-report.pdf. Accessed October 10, 2022. |
| 32. | Canadian Veterinary Medical Association. Expanding Veterinary Medicine Capacity 2022–2032: Report of the Canadian Veterinary Medical Association Veterinary Workforce Congress 2022. 2022. https://www.canadianveterinarians.net/media/5m1dvtwy/expanding-veterinary-medicine-capacity-in-canada-2022-2032-final.pdf. Accessed May 16, 2023. |
| 33. | Statistics Canada. Immigrants Make up the Largest Share of the Population in Over 150 Years and Continue to Shape Who We Are as Canadians. https://www150.statcan.gc.ca/n1/daily-quotidien/221026/dq221026a-eng.htm. Accessed June 30, 2023. |
| 34. | Statistics Canada. Canada at a glance: Racialized groups. 2022. https://www150.statcan.gc.ca/n1/pub/12-581-x/2022001/sec3-eng.htm. Accessed June 23, 2023. |
| 35. | Schurer JM, Phipps K, Okemow C, Beatch H, Jenkins E. Stabilizing dog populations and improving animal and public health through a participatory approach in Indigenous communities. Zoonoses Public Health. 2015;62(6):445–455. doi: 10.1111/zph.12173 |
| 36. | Statistics Canada. Income of Men and Women, Sub-Provincial Regions. https://www150.statcan.gc.ca/n1/pub/71-607-x/71-607-x2019006-eng.htm. Accessed December 18, 2023. |
| 37. | Daigneault PM, Birch L, Béland D, Bélanger SD. Taking subnational and regional welfare states seriously: insights from the Quebec case. J Eur Soc Policy. 2021;31(2):239–249. doi: 10.1177/0958928721996651 |
| 38. | Béland D, Dinan S, Rocco P, Waddan A. COVID-19, poverty reduction, and partisanship in Canada and the United States. Policy Soc. 2022;41(2):291–305. doi: 10.1093/polsoc/puac002 |
| 39. | Arluke A. Coping with pet food insecurity in low-income communities. Anthrozoos. 2021;34(3):339–358. doi: 10.1080/08927936.2021.1898215 |
| 40. | Ly LH, Gordon E, Protopopova A, Ly LH. Exploring the relationship between human social deprivation and animal surrender to shelters in British Columbia, Canada. Front Vet Sci. 2021;8:1–18. doi: 10.3389/fvets.2021.656597 |
| 41. | Humane Canada. National Pet Food Bank Program. c2022.https://humanecanada.ca/national-pet-food-bank/. Accessed June 9, 2023. |
| 42. | International Council for Veterinary Assessment. NAVLE. c2023. https://www.icva.net/navle/. Accessed July 2, 2023. |
| 43. | American Veterinary Medical Association. ECFVG Relationship with the Canadian NEB. 2015. https://www.avma.org/education/ecfvg/ecfvg-policies-and-procedures/ecfvg-relationship-canadian-neb. Accessed July 2, 2023. |
| 44. | Burkinshaw. Income Inequality in Canada. 2022:1–33. https://www.bankofcanada.ca/2022/07/staff-discussion-paper-2022-16/. Accessed September 5, 2022. |
| 45. | Card C, Epp T, Lem M. Exploring the social determinants of animal health. J Vet Med Educ. 2018;45(4):437–447. doi: 10.3138/jvme.0317-047r |
| 46. | Human Animal Support Services. A Community-First Movement to Serve People and Pets Equally. 2023. https://www.humananimalsupportservices.org/. Accessed August 21, 2023. |
| 47. | Humane Canada [Canadian Federation of Humane Societies]. Humane Societies and SPCAs in Canada: A Comprehensive Look at the Sector. 2016. https://humanecanada.ca/wp-content/uploads/2020/03/CFHS-Sector_Report_-_EN_-_Final.pdf. Accessed January 11, 2024. |
| 48. | Veterinary Services in Canada – Market Size, Industry Analysis, Trends and Forecasts (2023–2028). 2023. https://www.ibisworld.com/canada/market-research-reports/veterinary-services-industry/. Accessed December 18, 2023. |
| 49. | Reese L, Li X. Animal welfare deserts: human and nonhuman animal inequities. Front Vet Sci. 2023;10:1–12. doi: 10.3389/fvets.2023.1189211 |
| 50. | Canadian Institute for Healthcare Information. Canadian COVID-19 Intervention Timeline. 2022. https://www.cihi.ca/en/canadian-covid-19-intervention-timeline. Accessed June 29, 2023. |
Footnote
a In that and the current, study, pets are defined as dogs and cats.